

Abstract
OBJECTIVE To evaluate the efficacy of rituximab combined with CHOP-like regimen with or without IFN in patients newly diagnosed diffuse large B-cell Non-Hodgkin’s lymphoma (DLBCL).
METHODS From January 2003 to July 2008, 51 patients received CHOP-like chemotherapy (cyclophosphamide 750 mg/m2, epirubicin 80 mg/m2, vindesine 2.8 mg/m2 on day 1, and prednisolone 100 mg/day on day 1 to day 5). Thirty-one patients received CHOPR-like treatment (rituximab 375 mg/m2 1 day before CHOP-like chemotherapy). Twenty patients received CHOP-like regimen in combination with peginterferon (pegIFN) (1 μg/kg on day 5) and rituximab (on day 6).
RESULTS The CR (complete remission) rate in the CHOPR-like (with or without pegIFN) group and in the CHOP-like group was 78.4% and 45.1% (P = 0.005), respectively. The estimated mean time of overall survival (OS) in the CHOPR-like group and CHOP-like group was 58.7 ± 2.8 and 36.4 ± 3.4 months, respectively (P = 0.002). The rates of CR and OR (overall remission) in CHOPR-like with IFN arm were 85.0% and 95.0%, and the rates of those in CHOPR-like without IFN arm were 74.2% and 87.0% (P > 0.05). The estimated mean time of 4-year-PFS (progression-free survival) in CHOPR-like with IFN arm and in CHOPR-like without IFN arm was 62.9 ± 3.0 months and 51.0 ± 4.6 months (P = 0.092), respectively. In the CHOPR-like with IFN arm, no patient relapsed after achieving CR, while the estimated rate of 4-year-DFS (disease-free survival) in the patients who reached CR in the CHOPR-like without IFN arm was (63.4 ± 19.3)% (P = 0.061).
CONCLUSION Rituximab combined with CHOP-like chemotherapy improved the prognosis of DLBCL patients. The IFN may help to improve the quality and duration of response of DLBCL patients treated with rituximab and CHOP-like regimen.
keywords
Introduction
Rituximab is a chimeric monoclonal antibody that targets the B-cell-specific surface antigen CD20. CD20 is widely expressed on malignant B-cells, including indolent follicular lymphoma and aggressive diffuse large B-cell lymphoma (DLBCL). Diffuse large B-cell lymphoma accounts for approximately 40%-50% of new cases of adult lymphoma patients in China[1,2]. The addition of the anti-CD20 chimeric antibody rituximab to conventional chemotherapy, including the CHOP regimen, represents the most significant improvement in the treatment of B-cell lymphoma in the past 25 years[3]. In a retrospective analysis of the effects of this changed way in practice pattern, the 2-year progression-free (PFS, 69% vs. 51%) and overall survival (OS, 78% vs. 52%) proportions were significantly higher compared with CHOP in the period of prior to incorporation of rituximab[4,5]. Interferon alpha (IFN), which has multiple immunomodulatory effects, is an active agent for the indolent lymphoma at advanced stage. Some data obtained in vitro suggest synergistic activity of IFN with rituximab, via upregulation of CD20 and the enhancement of antibody-dependent cell-mediated cytotoxicity. Clinical trials have reported that, in patients with indolent lymphoma,the rates of both overall remission (OR) and the median duration of remission are higher in the patients receiving the treatment of combining immunotherapy employing rituximab and IFN with CHOP regimen than those with rituximab alone[5-7]. Bertè et al.[8] also reported the use of interferon-α in combination with rituximab was effective and well tolerated in relapsed and refractory DLBCL. However the result of another study showed IFN (Peginterferon alpha 2b, pegIFN) had no effect on upregulation of CD20 expression in peripheral lymph node tumor cells[9].
In the present study, we evaluated the efficacy of rituximab combined with CHOP-like regimen with or without IFN in Chinese patients with newly diagnosed DLBCL.
Materials and Methods
Patients and treatment protocol
The retrospective study included patients, age of 18 or more years old, who were newly diagnosed with CD20-positive DLBCL according to the World Health Organization (WHO) classification[10] and admitted to our hospital between January 2003 and July 2008. Patients were required to have no cardiac contraindications to doxorubicin therapy, no human immunodeficiency virus infection, and no prior neoplasm. They were required to have normal kidney and liver function proved by the test of serum biochemistry. The results showed as the followings: less than 2.0 mg/dl of total serum bilirubin, not more than twice of the upper limit of aspartate aminotransferase and alkaline phosphatase, less than 2.0 mg/dl of serum creatinine. Prior to treatment, patients were classified using the International Prognostic Index (IPI)[11]. The performance of the classification was assessed according to Eastern Cooperative Oncology Group (ECOG) criteria. The stage of the disease was assessed using the Ann Arbor system. Staging procedures included clinical examination, thoracic and abdominal computerized tomography (CT), blood count, bone marrow biopsy, and an echocardiograph examination measuring left ventricular ejection fraction. The urine pregnancy test for women of child-bearing age was examined in order to exclude the possibility of pregnancy. The study was approved by the ethics committee of research, and informed consent was obtained from all patients.
The treatment protocol consisted of the administration of 4-8 cycles of CHOP-like regimen. Each cycle included 21 days: cyclophosphamide 750 mg/m2; epirubicin 80 mg/m2; vindesine 2.8 mg/m2 (maximum 4 mg) on day 1; and prednisolone 100 mg/day on day 1 to day 5 and 16 days rest. Treatment could be postponed for 7 days if severe bone marrow suppression or severe infection occurred. Rituximab and IFN treatments were not randomized, but were dependent on the economic circumstances of the patients. Rituximab 375 mg/m2 was given through a slow infusion (according to the manufacturer’ s guidelines) 1 day before CHOP-like chemotherapy. When rituximab was combined with IFN, peginterferon alpha-2b (pegIFN) 1 μg/kg was given subcutaneously on day 5 and rituximab was given on day 6. Involved-field radiotherapy (36-40 Gy) was given combined with 4-6 cycles of chemotherapy in the patients in stage I or II. Patients who showed no response to the treatment after 4 cycles, received a second chemotherapy protocol. All other patients (advanced stage) received 6 to 8 cycles of chemotherapy, depending on the rate of response, and following that at least two cycles were given after maximum response. Granulocyte colony-stimulating factor (5 mg/kg) was administered subcutaneously daily starting from the first day when the neutrophil count fell below 0.5 × 109/L until it rising above 2.0 × 109/L. In the patients older than 70 years old, or those who experienced very severe complications, the dose of cyclophosphamide, epirubicin, and vindesine were reduced by 20%. If neutropenia persisted, the next scheduled cycle was postponed for one week; but the doses of rituximab and IFN were not modified. Patients also received support treatment with 10-20 g immunoglobulin intravenously for every cycle.
Evaluation criteria
Toxicity was evaluated on day 1 of every cycle by interview, physical examination and complete blood cell count. Hematologic and extra-hematologic toxicities were scored according to WHO criteria. The procedures for evaluation of the response were the same as those used for staging at diagnosis. CR was defined as an absence of clinical symptoms and signs. Partial remission (PR) was defined as the decrease in sum of the products of the greatest diameters (SPD) of tumors ≥ 50%. Progression of disease (PD) was defined as either an increase in SPD of tumors ≥ 50% or the presence of new clinical signs. Stable disease (SD) was defined as either an increase or decrease in SPD of tumors < 50%[12].
Statistical analysis
OS was calculated from the date of beginning chemotherapy to the date of death by any cause. PFS was calculated from the date of beginning chemotherapy to the date of progression or death from NHL. Disease-free survival (DFS) was defined as the time from the achievement of complete remission to the observation of relapse disease. Survival rates were calculated according to the Kaplan-Meier method, and differences between survival curves were evaluated using the log-rank test.
Results
Patient characteristics
Our study included 111 patients with newly diagnosed CD-20 positive DLBCL, who had been admitted to our hospital between January 2003 and July 2008. Among them, 9 patients were excluded in this study because of refusing further treatment in our hospital after the first cycle of therapy. Among the remaining 102 patients, 51 received CHOP-like treatment and 51 received CHOPR-like (CHOP-like + rituximab). Twenty out of the 51 patients also combined the CHOPR with IFN and the 31 without. A total of 269 (average 5.3) scheduled courses in CHOP-like group, 165 (average 5.3) in CHOPR-like without IFN, and 93 (average 4.7) in CHOPR-like with IFN were administered and finished.
Clinical characteristics of the patients at the time of diagnosis are shown in Table 1. There were major imbalances in prognostic factors in the three cohorts. The CHOP-like group overall had better prognostic features. Rituximab and IFN treatments were not randomized, but were mainly dependent on the economic circumstances of the patients. Otherwise, we were inclined to administer rituximab and IFN to those with the worst IPI.
Baseline characteristics of study populations.
Response and follow-up
The responses of patients to CHOP-like or CHOPR-like treatment are shown in Table 2. The CR and OR (CR + PR) rates were statistically higher in the CHOPR-like group than those in the CHOP-like group. The disease in progression was shown in 39.2% of patients in the CHOP-like (received 3.7 average cycles) group, but presented in 9.8% of patients treated with CHOPR-like regimen (received 3.6 average cycles) only.
Response to treatment of CHOP-like or CHOPR-like, %.
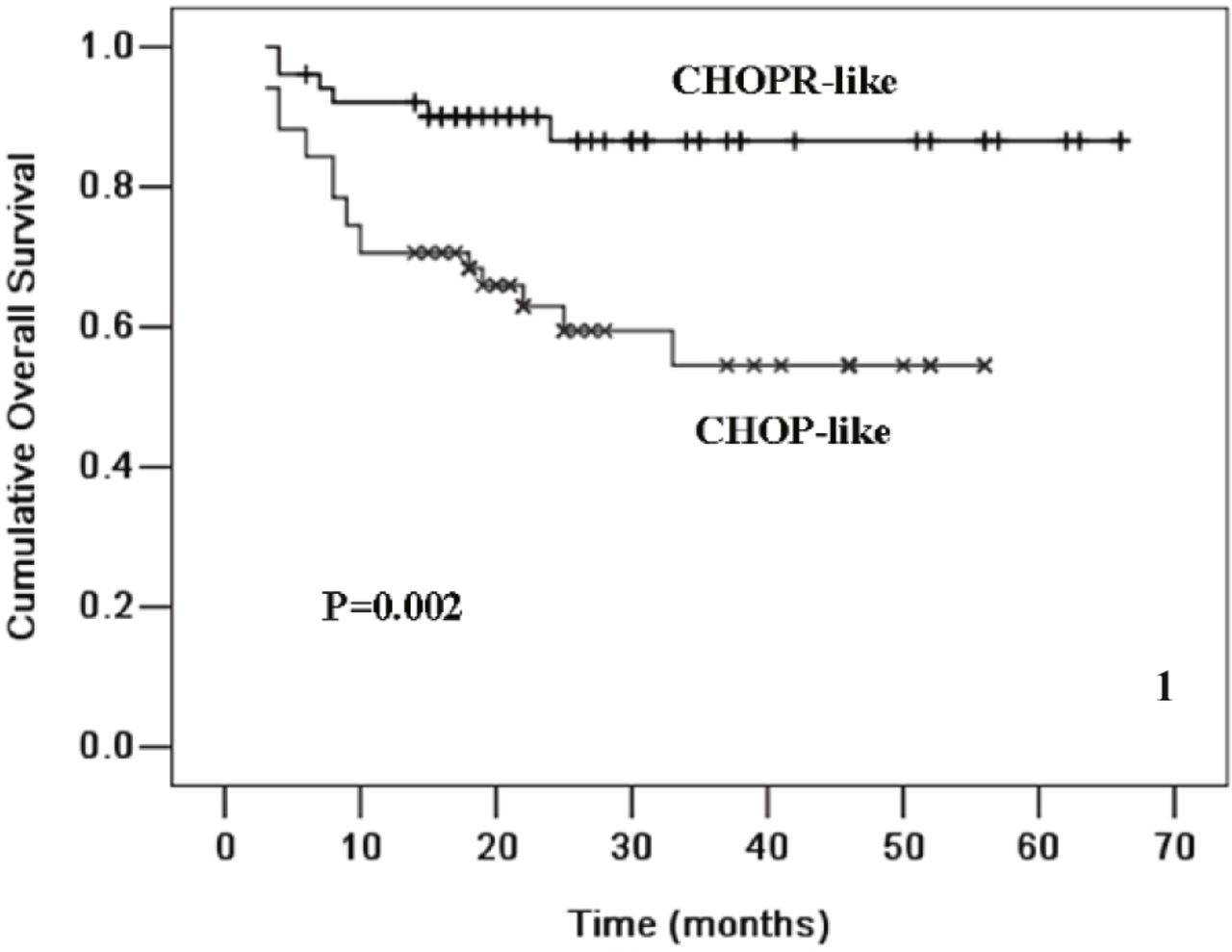
The estimated mean time of OS in the CHOPR-like group and in the CHOP-like group was 58.7 ± 2.8 months and 36.4 ± 3.4 months, respectively; and the rate of 4-year OS in the CHOPR-like and CHOP-like groups was (86.6 ± 5.3)% and (54.5 ± 8.4)%, respectively (P = 0.002, Fig. 1). The estimated mean time of PFS in the group of CHOPR-like was 55.2 ± 3.3 months and 30.6 ± 3.6 months in CHOP-like group. The rate of 4-year PFS in the groups of CHOPR and CHOP was (80.1 ± 6.1)% and (40.6 ± 9.7)%, respectively (P = 0.001, Fig. 2).

Kaplan-Meier plot of OS for DLBCL patients treated with CHOP-like (n = 51) and those with CHOPR-like (n = 51).
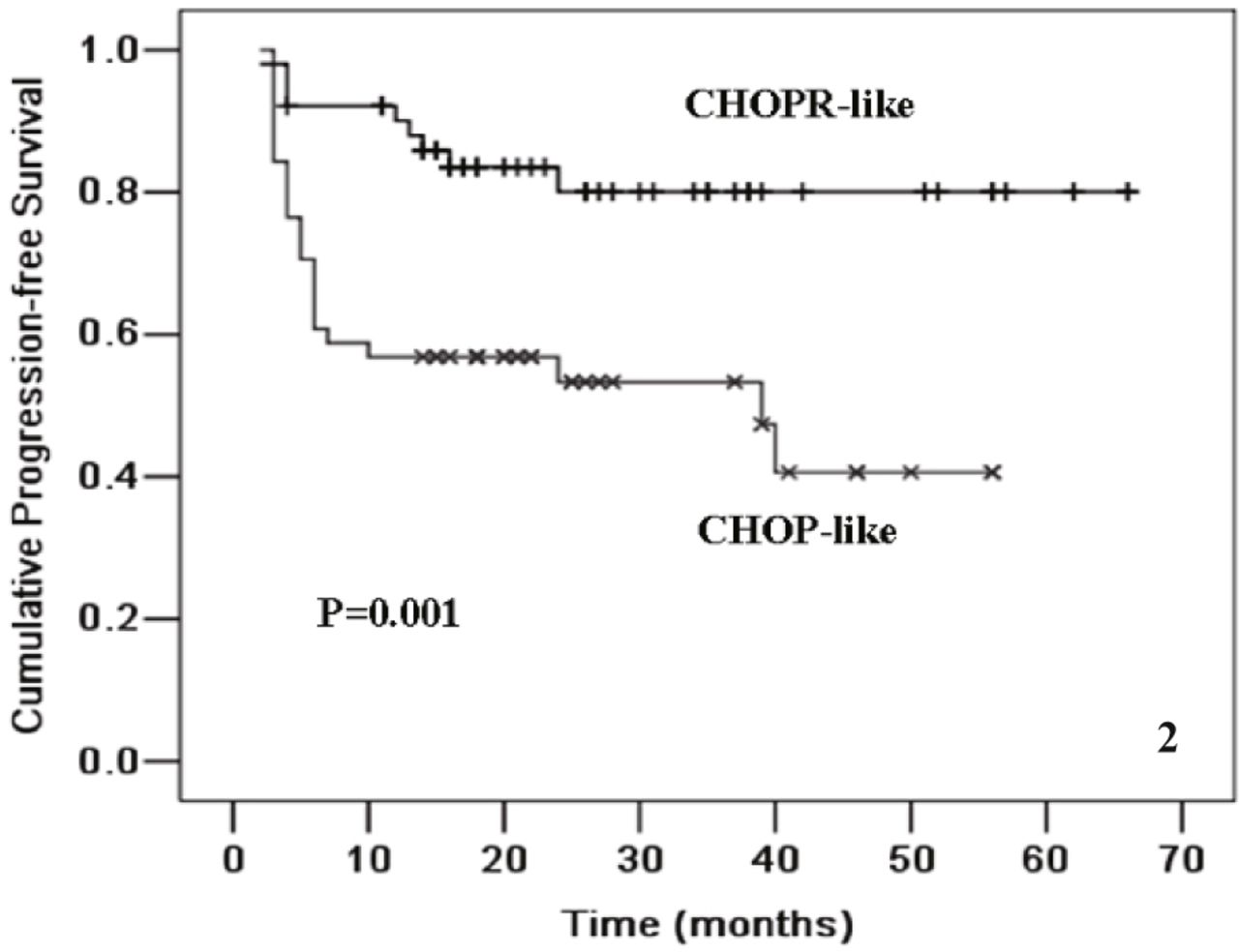
Kaplan-Meier plot of PFS for DLBCL patients treated with CHOP-like (n = 51) and those with CHOPR-like (n = 51).
When patients received CHOPR-like with IFN treatment, 85.0% (17/20) of them achieved CR, with an OR rate of 95.0% (19/20). Among the patients who received CHOPR-like without IFN treatment, 74.2% (23/31) of them achieved CR and the OR rate was 87.0% (27/31). The differences in CR and OR rates between these 2 groups were not statistical significant (Table 3). The mean time of follow-up for the patients treated with and without IFN was 28 months (ranging from 4 to 66 months) and 30 months (ranging from 4 to 66 months), respectively. In patients with and without IFN, the estimated rate of 4-year OS was (89.7 ± 6.9)%, and (84.9 ± 7.2)%; and the estimated mean time of OS was 59.8 ± 4.2 and 58.2 ± 3.6 months, respectively (P = 0.836). The estimated 4-year PFS in the patients with and without IFN was (95.0 ± 4.9)% and (72.1 ± 8.6)%, respectively; and the estimated mean time of PFS in the patients with and without IFN was 62.9 ± 3.0 and 51.0 ± 4.6 months, respectively (P = 0.092, Fig. 3). In the group of CHOPR-like with IFN arm, no patient relapsed after achieving CR, while among patients treated with CHOPR-like without IFN, the estimated rate of DFS was (63.4 ± 19.3)% (P = 0.061, Fig. 4).
Response to treatment of CHOPR-like with or without IFN, %.
Adverse effects in patients treated with CHOP-like or CHOPR-like regimen (n = 102).
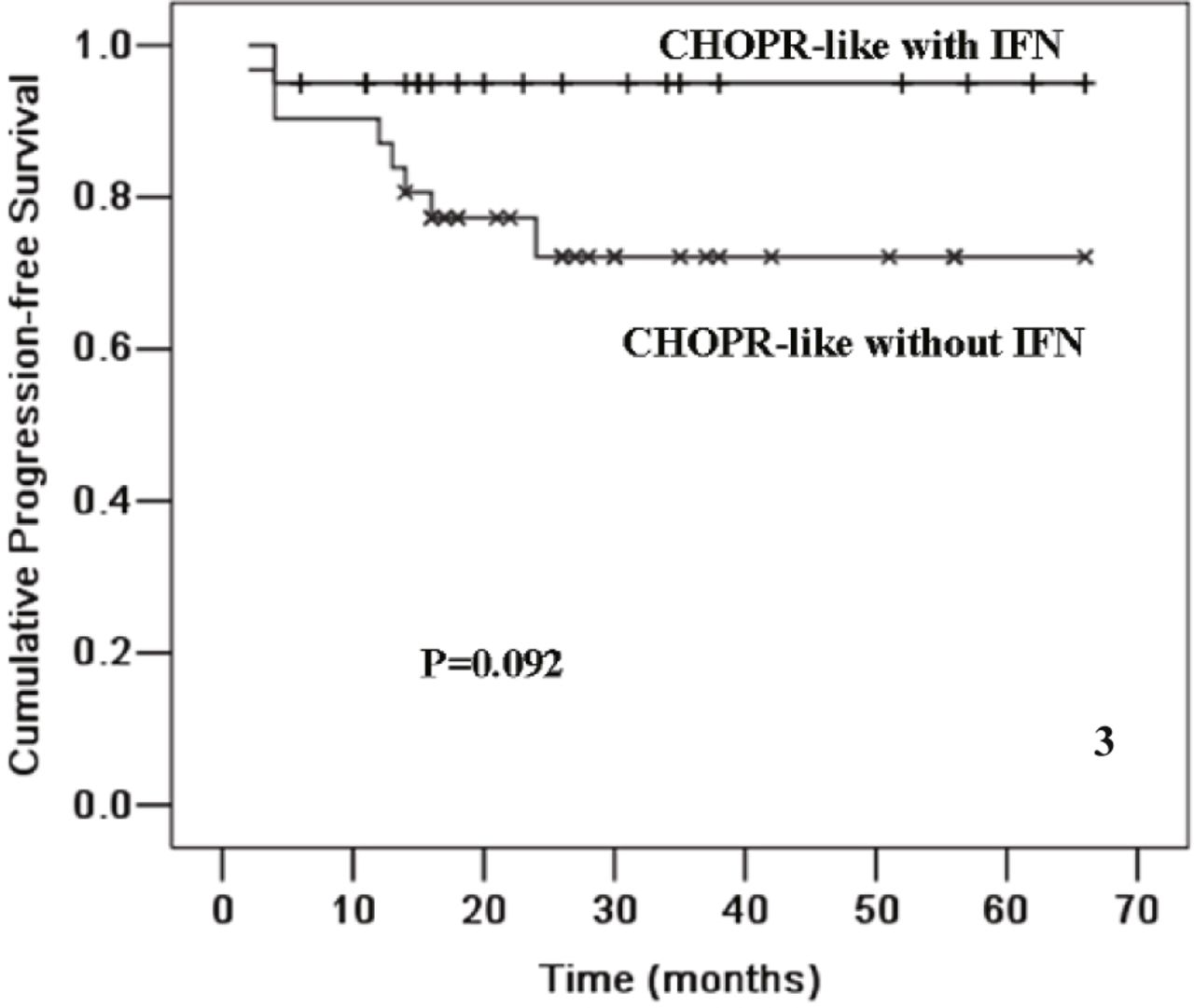
Kaplan-Meier plot of PFS for DLBCL patients treated with CHOPR-like with IFN (n = 20) and those without IFN (n = 31).

Kaplan-Meier plot of DFS in CR patients treated with CHOPR-like with IFN (n = 17) and those without IFN (n = 23).
Toxicity
Mild rituximab-infusion-related occurred in approximately 25% of the patients, primarily during the first time of rituximab infusion. The reactions included chills, rigor, and hypotension. However, such symptoms were mild, and resolved when the infusion rate was reduced. Influenza-like symptoms, such as fatigue, fever, and muscular soreness, occurred in 30% (6/20) of patients treated with IFN, which could be relieved by acetominophen quickly. Hematologic toxicities, including neutropenia, anemia, and thrombocytopenia in CHOP-like group were similar with those in CHOPR-like group. The differences in the rates of these complications happened between the patients treated with-IFN and without-IFN were not significant. Although the support treatment of intravenous immunoglobulin was given, 50% of patients treated with CHOPR-like had a decreased serum immunoglubin (Ig) levels, while 19.6% of patients treated with CHOP-like were decreased in their Ig levels (P < 0.05). And 35.0% of the patients treated with-IFN and 58.1% patients treated without-IFN arms had decreased Ig levels (P > 0.05). However, we observed no significant increasing rate in the infection induced by these decreased Ig levels in the CHOPR-like group. The most important non-hematologic toxicity was the liver injury, especially in the patients with positive HBV markers. After the rituximab treatment, two patients with chronic hepatitis B in latent phase experienced a reactivation of HBV infection. One patient treated with CHOPR-like with IFN died of severe hepatic insufficiency; and the condition of the other improved following liver protective measures. One patient treated with CHOPR-like with IFN died of severe lung infection. All other deaths occurred because of disease progression.
Discussion
DLBCL is the most prevalent type of NHL diagnosed in Chinese patients. The standard treatment for many years has been CHOP chemotherapy. The rates of OR and CR generally achieves approximately 70%-90% and 40%-60%, respectively. Rituximab combined with CHOP chemotherapy has been proven to have high effects in the treatment of DLBCL[13-17]. Since 2003, when rituximab was introduced into our hospital, we have applied the regimen of combining CHOP with rituximab to treat DLBCL patients. Several clinical trials have shown that combining the immunotherapy of IFN with rituximab is able to improve the OR rate and the median duration of remission in indolent lymphoma[6,7]. To determine whether the synergistic effects between IFN and rituximab may operate in the treatment of DLBCL, we began, in some patients, to add IFN before the infusion of rituximab. The patients who received IFN were those who could afford for the treatment. From January 2003 to July 2008, 51 patients completed at least 4 cycles of CHOP-like chemotherapy combined with rituximab. Among them, 20 patients received pegIFN injection before rituximab infusion. We have demonstrated here the efficacy of CHOPR-like (with or without IFN) as the first-line treatment of DLBCL in Chinese patients: CR rate achieving 78.4%, OR rate being 90.2%, and an estimated rate of 4-year OS achieving (86.6 ± 5.3)%, while the rate of CR and OR in homeochronous patients treated with CHOP-like was 45.1% and 58.8%, respectively, and the estimated rate of 4-year OS was (54.5 ± 8.4)%.
We then set out to determine whether IFN can improve the efficacy of CHOPR-like. Our results showed that the rates of CR and OR in the patients treated with IFN were slightly higher than those in the patients treated without IFN, but the difference was not statistically significant. The estimated 4-year PFS in the IFN arm was higher than that in the control arm [(95.0 ± 4.9)% vs. (72.1 ± 8.6)%], and the estimated mean time of PFS in the group with IFN arm was 12 months longer than that in the group without IFN. Thus, pegIFN injection before rituximab infusion appeared to improve the efficacy of CHOPR-like in the treatment of DLBCL. There was some indication that pegIFN treatment extended PFS time, although, perhaps due to the limited number of cases studied, these differences were not statistically significant.
Our most significant finding has been that, to date, none of the patients in the IFN arm who achieved CR has relapsed, whereas the estimated DFS rate among patients who received CHOPR-like without IFN was (63.4 ± 19.3)% (P = 0.061). This suggests that pegIFN injection before rituximab infusion may improve the quality of CR and reduce the possibility of relapse in DLBCL patients who achieve CR after CHOPR-like treatment with IFN. No additional adverse effects were observed in the IFN arm other than influenza-like symptoms.
Although the mechanism of action of rituximab is not completely defined, the antibody binding human C1q and affecting both complement-dependent cytotoxicity and antibody-dependent cell-mediated cytotoxicity (ADCC) were considered. IFN-α is a pleiotropic cytokine and exerts various effects on the immune system, including modulation of immunoglobulin production, inhibition of T-suppressor cell function, stimulation of T-cell cytotoxicity, monocyte/macrophage functions, and natural killer cell activity, which is an integral part of ADCC. It is possible that the immunomodulatory effect of IFN-α and the rituximab-dependent cell-mediated cytotoxicity act synergistically to induce neoplastic clone suppression[18,19]. IFN is also known to upregulate neoplastic antigen expression on the surface of human carcinoma cells, and can augment the localization of monoclonal antibodies to the tumor site. In mice, IFN-α has been shown to have the ability to enhance tumor uptake of an anti-melanoma monoclonal antibody[20,21]. Studies in vitro have shown that IFN-α is able to induce overexpression of CD20 antigen on B-CLL-cells surfaces, which suggests that administration of IFN-α before and during rituximab treatment may be effective in enhancing the efficacy of this treatment[22,23]. A phase II randomized trial has shown that, among patients with symptomatic, advanced, indolent lymphoma who received CHOPR-like alone or in combination with IFN-α, significantly more of the patients receiving combination therapy improved their CR and maintained their response for more than 24 months. The addition of IFN to rituximab was generally safe, although reversible thrombocytopenia and neutropenia were noted in some patients[24].
The results of our study show that combining CHOP-like chemotherapy with IFN and rituximab is feasible and relatively safe in newly diagnosed DLBCL. This combination may increase CR and OR rates, and prolong the OS, and particularly the time of PFS and DFS. Since IFN seems to improve both the quality and duration of the response of DLBCL patients treated with CHOPR-like, we propose that randomized trials investigating CHOPR-like with or without IFN are needed. If these promising results are confirmed, combining chemotherapy with IFN and rituximab could be extended to previously untreated DLBCL patients. Combination of IFN and rituximab treatment may also be effective as a maintenance therapy to clear minimal residual disease after chemotherapy so as to prolong the duration of remission.
Conflict of interest statement
No potential conflicts of interest were disclosed.
Footnotes
This work was partly supported by grant from the Shanghai Science and Technology Committee, Shanghai, China (No. 064119511).
- Received December 13, 2008.
- Accepted March 4, 2009.
- Copyright © 2010 by Tianjin Medical University Cancer Institute & Hospital and Springer
References
In this issue






{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.