

Abstract
Colonic lipoma is an uncommon benign non-epithelial tumor of the gastrointestinal tract. It typically occurs in the ascending colon and among old female patients. Most cases are asymptomatic and do not require any special treatment. However, we encountered a young male patient with a symptomatic lipoma located in the transverse colon that induced a transcolocolonic intussusception. He presented with such symptoms as diarrhea, tenesmus, abdominal pain, and weight loss. Colonoscopy revealed a spherical polypoid lesion with partial congestion and ulceration on its surface, and the related biopsy revealed spindle cell hyperplasia and inflammatory cell infiltration. Reduction of the intussusception was not attempted, and transverse hemicolectomy was conducted. Although several novel techniques have been reported for the diagnosis and treatment of colonic lipoma, for our case patient, an exact diagnosis was made postoperatively via histological examination and laparotomy was performed.
keywords
Introduction
Lipoma of the colon is a rare condition that may be incidentally detected at colonoscopy, surgery, or autopsy. Most colonic lipomas are asymptomatic and do not require treatment. Herein, we report the case of a young male patient with a symptomatic lipoma located in the transverse colon that induced a transcolocolonic intussusception. Transverse hemicolectomy was then performed, and the exact diagnosis was made via postoperative histological examination.
Case Report
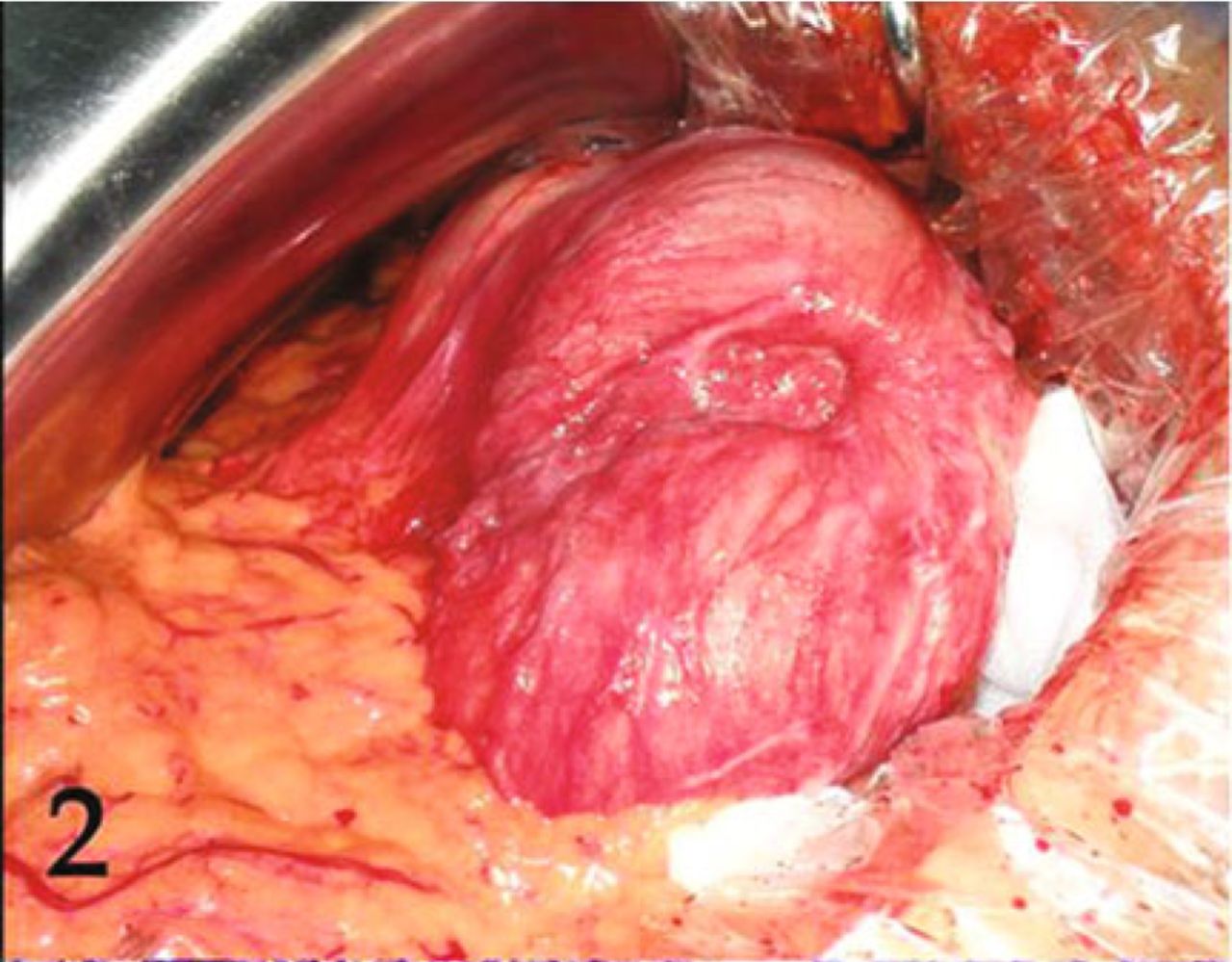
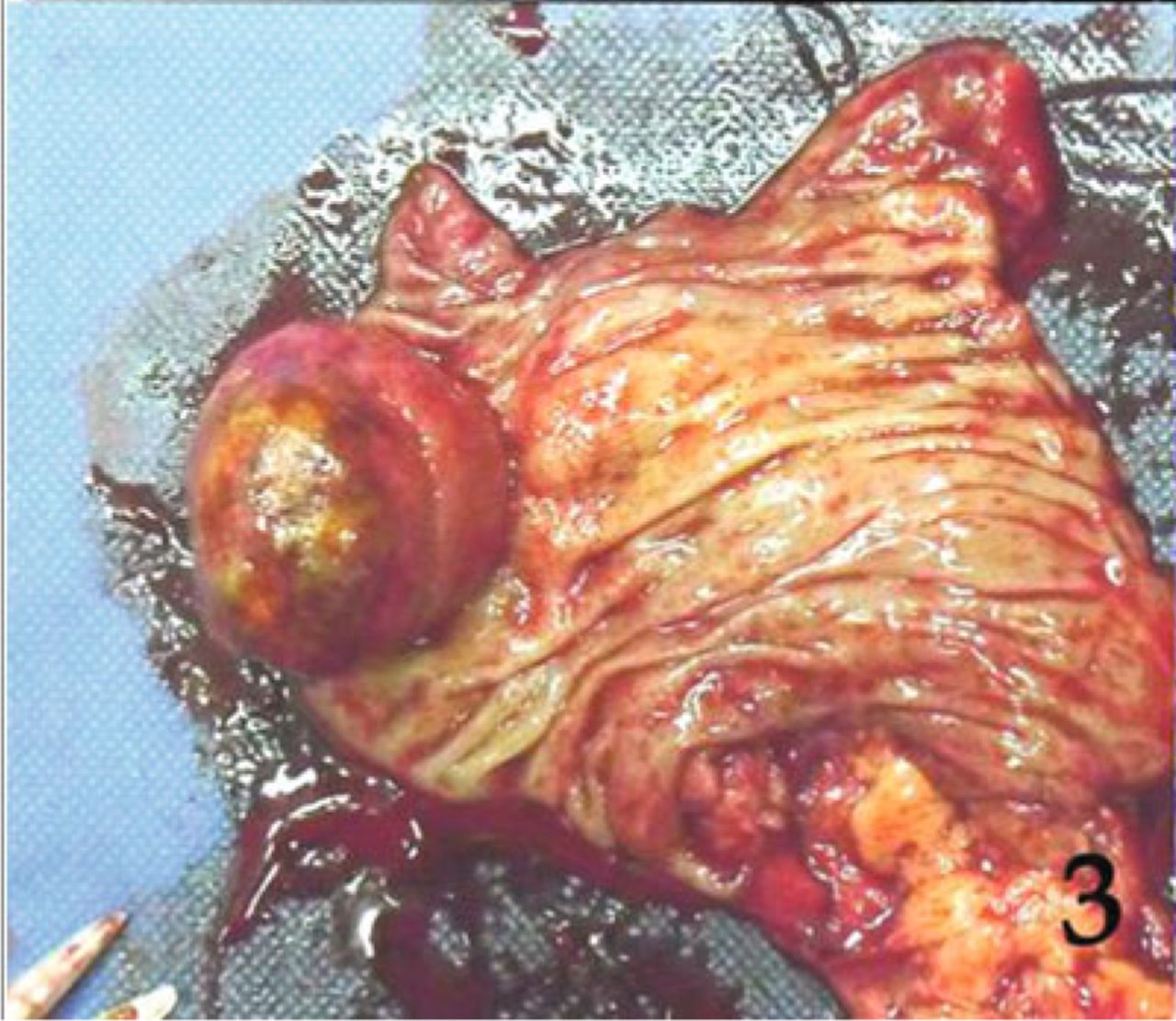
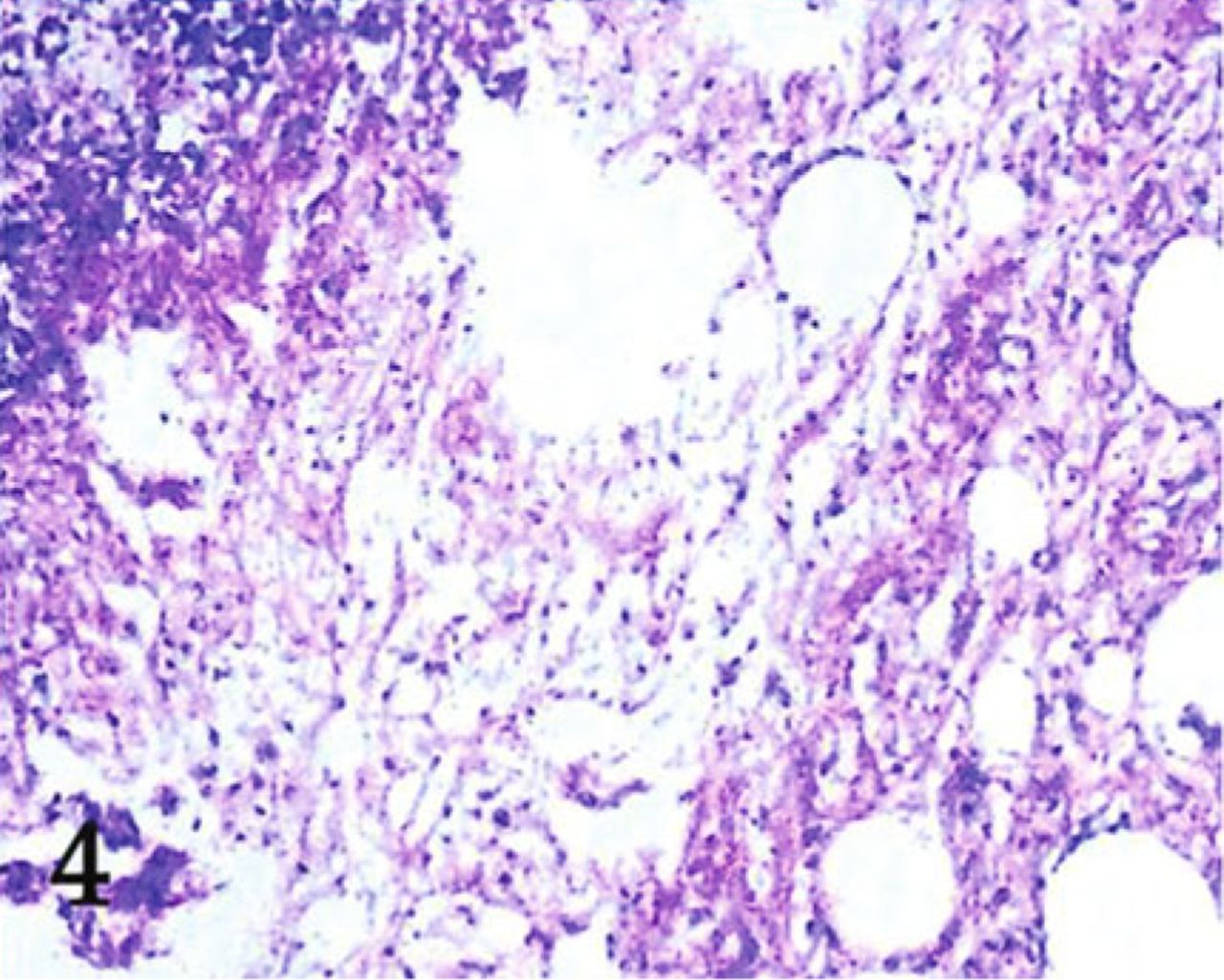
A 37-year-old man presented to us in February 2010 with complaints of 2 monthes’ duration of diarrhea with pasty stool, tenesmus, persistent abdominal pain, and distention. These symptoms became aggravated for the most recent half-month before the patient’s visit and were somewhat triggered by passes of gas and defecation. His physical examination was unremarkable. Enhanced computed tomography (CT) revealed an oval low-density lipoma(CT number, -94 HU) protruding into the lumen of the transverse colon and transcolocolonic intussusception (Fig. 1). Colonoscopy and biopsy were performed followed by laparotomy; a yellowish spherical polypoid lesion (3.8 cm×3.5 cm×3.7 cm) associated with partial congestion and ulceration on its surface was seen arising from the median of the transverse colon. The submucosal and sessile lesion was accompanied by transcolocolonic intussusception (Fig. 2). Reduction of the intussusception was not attempted, and transverse hemicolectomy was performed. Postoperative histological examination identified ulcerations on the surface of the tumor and a large quantity of maturate differentiated adipose cells on its subsurface, among which spindle cells and hyperplastic small vessels were found; hyperplastic spindle cells were also detected below the epithelium mucosae (Fig. 3). A pathological diagnosis of colonic lipoma was made (Fig. 4). Metastases to the lymph nodes were not discovered. The patient had an uneventful postoperative course and was discharged home a few days later.

Enhanced CT image showing an oval low-density tumor protruding into the lumen of the splenic flexure in the colon (CT number, -94HU). Intussusception induced by the colonic lipoma was also detected.

Transverse colon intussusception.

Resected colon segment showing a bright yellow sessile and submucosal tumor measuring 3.8 cm×3.5 cm×3.7 cm.
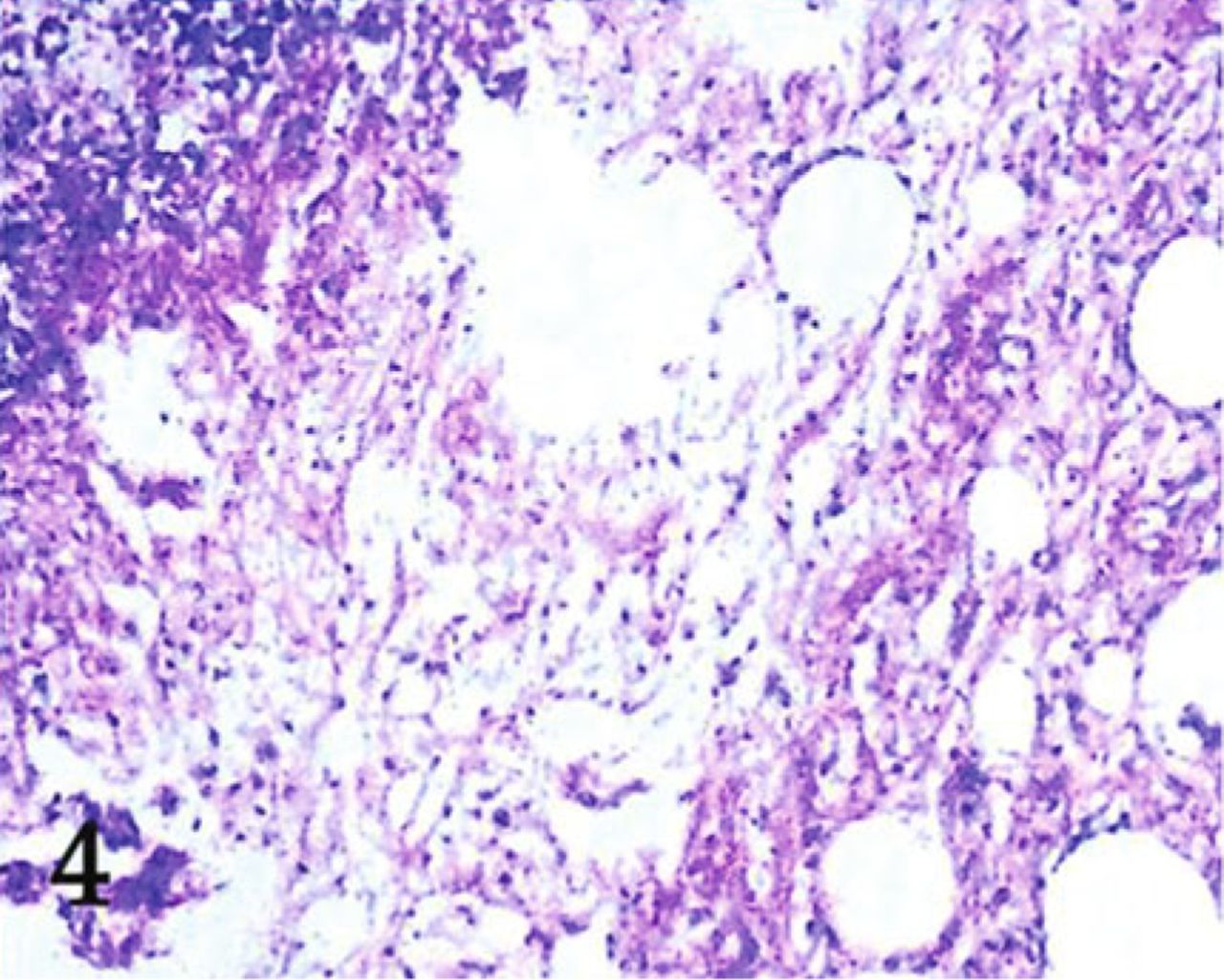
Postoperative histological examination revealed a large quantity of maturate differentiated adipose cells on the subsurface of the tumor, among which spindle cells and hyperplastic small vessels were found (H&E stain; original magnification, ×100).
Discussion
Lipoma of the gastrointestinal tract was first described by Bauer et al.[1] in 1757. Its incidence has been reported to range between 0.2% and 4.4%, and it accounts for 2.6% of all gastrointestinal benign tumors[2]. The median age of patients at the time of diagnosis ranges from 50 to 69 years. Most colonic lipomas occur in the cecum and ascending colon[3]. Colonic lipomas generally do not cause symptoms, and only a minority of lipomas can cause symptoms when the lesion is large[3]. Their most common signs and symptoms include abdominal pain, bleeding per rectum, and alterations in bowel movements[4]. They may also occur, albeit rarely, with such dramatic presentations as massive hemorrhage, intussusception, or even perforation, for which emergency operation is required. The present case is quite exceptional as it involves a young male patient with a symptomatic lipoma located in the transverse colon that induced intussusception due to its size.
Various clinical and imaging methods have been described for the diagnosis of colonic lipomas. CT is an excellent method for diagnosis based on the characteristic fatty densitometric features of lipomas[5]. However, a preoperative diagnosis mainly depends on colonoscopy because it can provide direct visualization and pathological examination via biopsy forceps. Typical lipomas appear as smooth, spheroidal, and slightly yellowish polyps of variable size, with or without a pedicle. Nevertheless, diagnosing lesions with an atypical, callous, or ulcerated shape may prove to be difficult. The preoperative and intraoperative diagnoses were both difficult to confirm in our case patient. We believe that postoperative pathological examinations are reliable for a definite diagnosis.
Once the removal of a colonic lipoma is considered necessary, it is generally accepted that lipomas up to 2 cm in diameter should be resected by endoscopic cautery snare and that those larger than 2cm should be removed surgically[6]. Some scholars agree to local enucleation; removal of colonic lipomas via laparoscopy has also been reported, but this practice is still associated with several problems and thus remains controversial.
Laparoscopic surgery was our first choice for our case patient, but he and his family requested a laparotomy instead for which we found local enucleation unsuitable and thus considered resection of the colon segment. Reduction of the intussusception was also not fitting due to the increased risk of perforation and anastomotic complications of the manipulated friable and edematous bowel tissue involved. In summary, the outcomes of this case suggest that intraoperative pathological examination of frozen tissue specimens is essential to rule out interstitial tumors, and we will use this valuable experience in our future work.
Conflict of Interest Statement
No potential conflicts of interest were disclosed.
Acknowledgements
This work was supported by the National Science Foundation of China (Grant Nos. 30972879 and 81172370), the Specialized Research Fund for the Doctoral Program of Higher Education (Grant No. 200801590006), and the Natural Science Foundation of Liaoning Province (Grant No. 20092129)
- Received August 14, 2011.
- Accepted October 13, 2011.
- Copyright © 2011 by Tianjin Medical University Cancer Institute & Hospital and Springer
In this issue






{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.