

keywords
Case Report
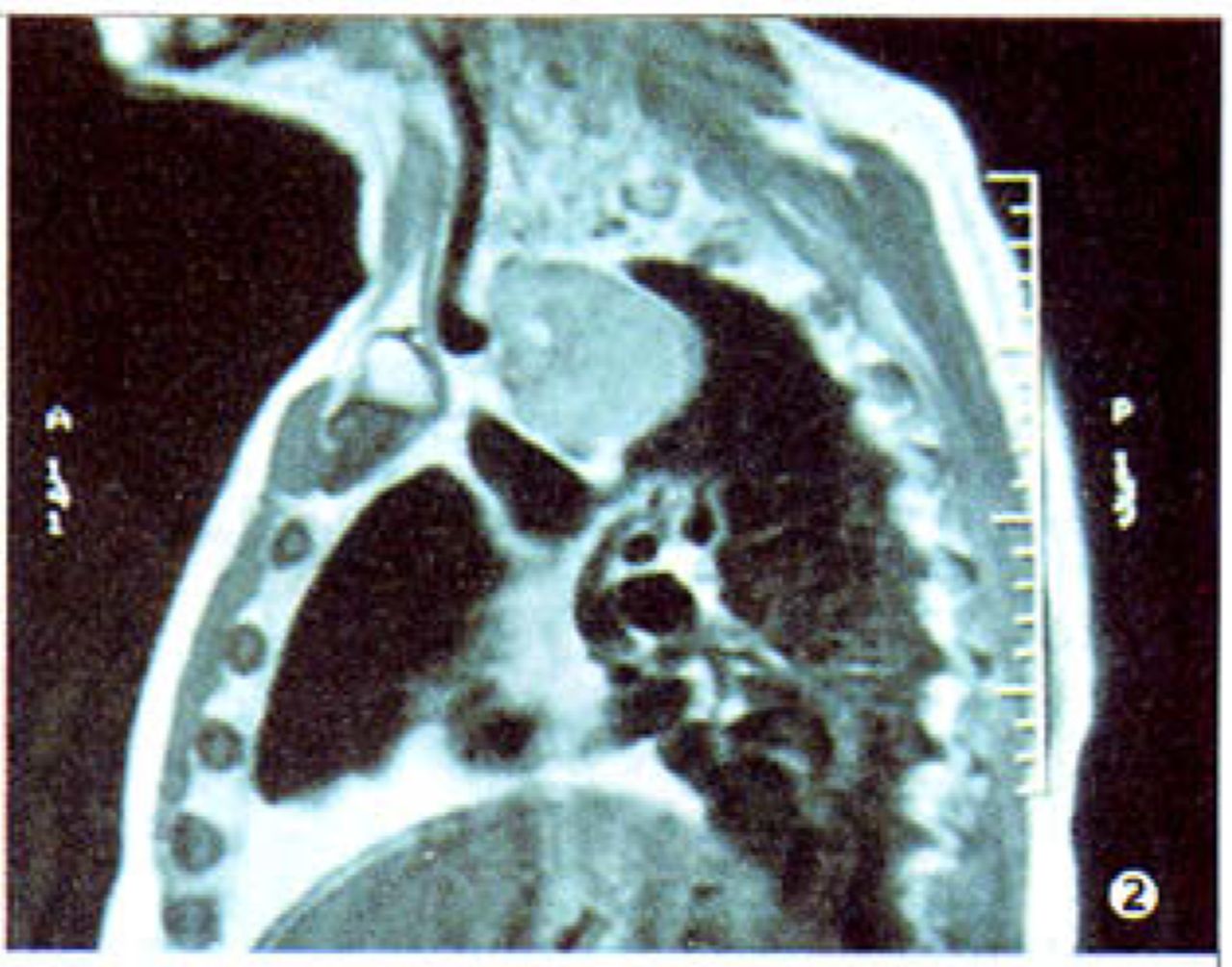
A 58-year-old male patient presented to our department for surgical management of a right neck nodule and low fever over the past 2 weeks. Preoperative evaluation, which included chest CT scan, MRI and scintigraphy (99mTc), revealed round and clear boundary intrathoracic ectopic thyroid tissue at the right side of the anterior mediastinum and an enlarged lymph node in the right neck. The preoperative general image diagnosis concluded a malignant ectopic intrathoracic goiter Figs.1~Figs.3 The lymph node biopsy confirmed a metastatic papillary adenocarcinoma of the thyroid.. The tumor was resected via a cervical collar incision Figs.4. Bilateral hemithyroidectomy and cervical lymph node dissection were also performed. We noticed that the intrathoracic thyroid was not connected to the cervical thyroid. Blood was supplied from the intrathoracic vessels, thereby establishing the diagnosis of an ectopic intrathoracic thyroid. Final pathologic diagnosis was a papillary adenocarcinoma of the thyroid in an ectopic intrathoarcic goiter with involved lymph node. The postoperative course was uneventful.

CT scan: mediastinal mass of inhomogeneous density.
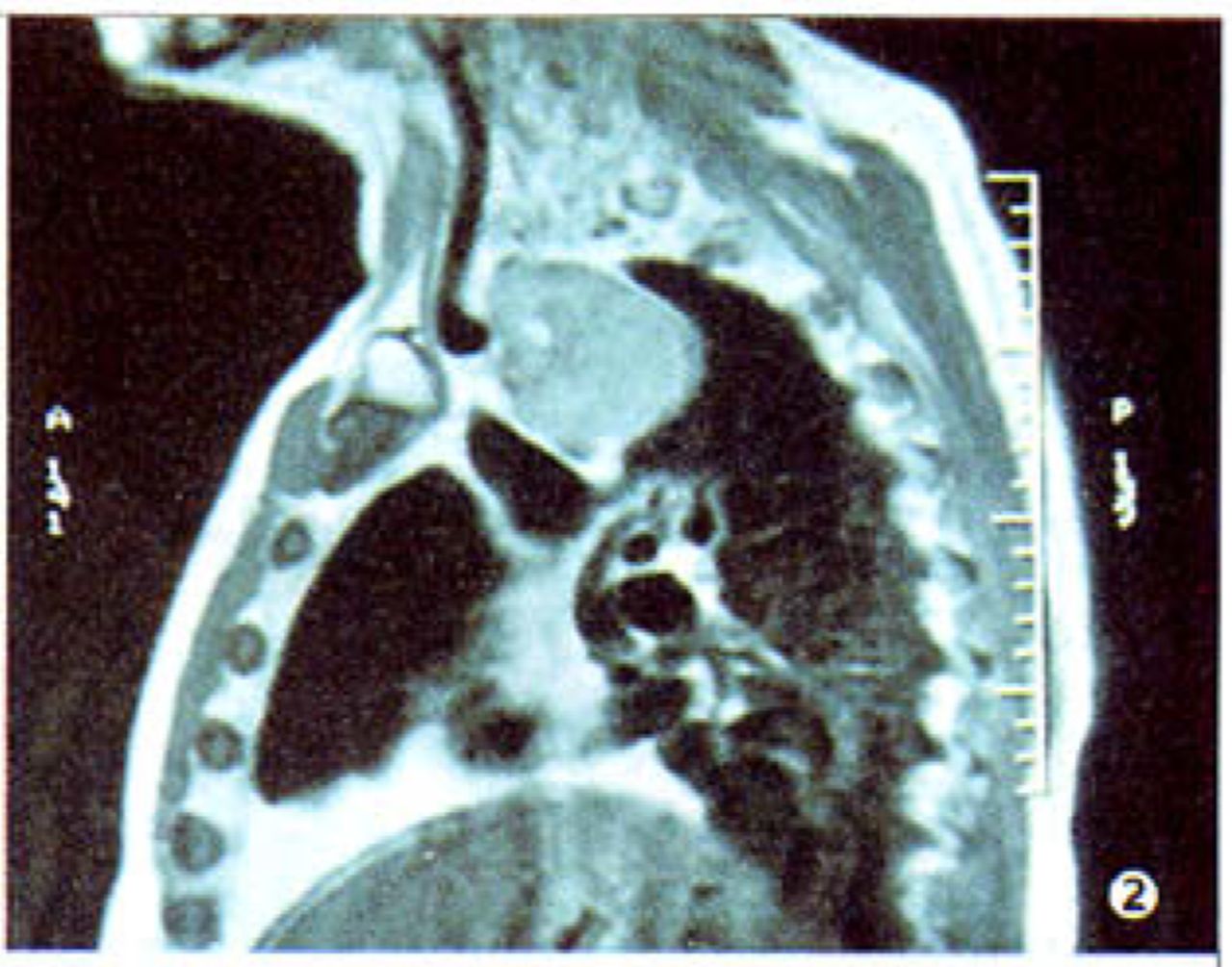
MRi: the mass with round and clear boundary.

Scintigraphy (®Tc) detected one additional thyroid lesion underlying the normal thyroid.

Specimen of the tumor, papilla can be seen inside the goiter.
Discussion
Retrosternal goiter is the result of progressive enlargement of the thyroid parenchyma, which extends behind the upper part of the sternum within the superior mediastinum. It is not uncommon in patients with a mediastinal tumor (5~7%).[1] Most substemal goiters are benign. The blood supply of a secondary intrathoracic goiter is from the superior and inferior thyroid arteries. The presence of ectopic intrathoracic thyroid tissue in the mediastinum is a very rare entity, called "primary intrathoracic goiter".[2] Chest computed tomography provides important information, with high sensitivity (98%), showing the location of the ectopic thyroid tissue and its relation with the great vessels and other structures in the mediastinum.[2,3] Scintigraphy is not always diagnostic, however, it may be useful when positive. The ectopic intrathoracic thyroid should be removed to rule out malignancy. Excision of this tissue is usually not possible through a cervical incision, and so a thoracotomy or sternotomy is sometimes required. This is a safe procedure with a very low mortality rate (0 ~2%) and an acceptable morbidity. Prognosis is excellent following a successful excision.[3]
- Received March 1, 2006.
- Accepted March 17, 2006.
- Copyright © 2006 by Tianjin Medical University Cancer Institute & Hospital and Springer
In this issue






{kind=link}
{kind=link}
{kind=link}
{kind=link}
Related Articles
Cited By...
- No citing articles found.