

Abstract
OBJECTIVE To assess the postoperative QOL (Quality of Life) of Chinese laryngeal cancer patients who have undergone a partial or total laryngectomy and to analyze their prognostic factors, as well as to assess the feasibility of using the University of Washington Quality of Life (UW–QOL) questionnaire in QOL studies of Iaryngeal cancer patients.
METHODS Using the UW–QOL questionnaire, a survey was conducted in patients treated by a partial or total laryngectomy for laryngeal cancer.
RESULTS Questionnaires were sent to 142 patients who were disease– free for more than half a year after surgery. Replies were received from 130 patients (91% response rate) with 118 patients completing the questionnaire. These patients were divided into 2 groups: a partial–laryngectomy group (n = 81; excluding cordectomy) and a total–laryngectomy group (n = 37). The composite QOL scores of the partial-laryngectomy group (692.3 ± 127.9) were higher than those of total-laryngectomy group (6364 ± 140.0), showing a statistically significant difference (P < 0.05). The partial-laryngectomy group (74.3 ± 23.8; 80.9 ± 20.3) was better than the total-laryngectomy group (40.3 ± 25.8; 696 ± 27.1) in speech and appearance (P < 0.001; P < 0.05) but the total–laryngectomy group (92.6 ± 13.0) was superior to the partial-laryngectomy group (83.0 ± 20.5) in pain (P < 0.01). Six factors including cancer stage, operative modality complications, postoperative radiotherapy or chemotherapy, living partners and chronic disease before or after operation were related to postlaryngectomy QOL.
CONCLUSION Partial laryngectomy is superior to total laryngectomy in speech, appearance and overall QOL. Besides operative morality, cancer stage, complications, postoperative radiotherapy or chemotherapy, Iiving partners and chronic diseases before or after operation are factors influencing postlaryngectomy QOL. As a whole, the UW–QOL questionnaire is a good instrument for studying QOL of laryngeal cancer patients in China, and it can be used to explore the QOL outcomes obtained from different reconstructive techniques.
keywords
With the development of medicine, the evaluation standards of surgical curative effect of laryngeal cancer have varied, shifting from survival rate alone to estimation of functional reconstruction and postoperative outcome.[1,2] Nowadays, the research on Quality of Life (QOL) of head and neck cancer patients has grown and has moved to making the evaluation more comprehensive and objective. [1,2] Although it was initiated abroad in the 1950’s and has developed rapidly since then, this is not the case in China, and no specific research in China on the QOL in laryngeal cancer patients has been reported.
In the past 20 years, even patients with Stage I laryngeal cancer were treated by total laryngectomy, which severely impaired their appearance and important functions including speech and swallowing. Recently, the development of functional laryngeal surgery not only has helped to preserve functions, but also has made the postoperative survival rate equal to total laryngectomy at the same stage of cancer.[3] However, with the new surgery, there is a relatively high occurrence of complications, such as aspiration and stenosis of the larynx. Intuitively, the QOL of the patients undergoing partial laryngectomy seems to be better than that of those undergoing total laryngectomy, but it has not been demonstrated with QOL research. Therefore, the purpose of our study was to determine with QOL research whether the postoperative QOL of the patients undergoing partial laryngectomy was better than those undergoing total laryngectomy, and if so, in addition to operative modalities, which factors influence the postoperative QOL of laryngeal cancer patients.
To answer these questions in this retrospective study, we employed the University of Washington-Quality of Life (UW-QOL) questionnaire. We assessed and compared the postoperative QOL of laryngeal cancer patients who underwent either partial or total laryngectomy, and analyzed the factors influencing postoperative QOL.
Materials and Methods
Participants
Candidates for the study consisted of patients with laryngeal cancer confirmed by pathology, who had been treated by either partial or total laryngectomy in the Department of Otorhinolaryngology of the First Hospital of China Medical University between January 1999 and April 2005 and who had completed more than a half a year of follow-up. Patients were excluded from the study on basis of the following criteria: 1) presence of a second primary tumor before or after operation; 2) death, recurrence or metastasis of a cancer after operation; 3) failure to follow-up. This procedure yielded 234 patients, of whom 142 were asked to complete a questionnaire by themselves through the mail or by a clinic inquiry. Of these patients, 130 returned the questionnaire, giving a response rate of 91%. Twelve of the patients who participated were excluded because they returned only partially completed questionnaires. The data from the remaining 118 patients were used in the study. These patients were divided into 2 groups: a partial-laryngectomy group (n=81; excluding cordectomy) and a total-laryngectomy group (n=37), whether or not accompanied by bilateral or unilateral neck dissection. The details of clinical information of the patients are shown in Table 1.
QOL assessment
The revised edition of UW-QOL questionnaire was administered in our study.[4] The UW-QOL questionnaire is a self-administered scale consisting of 9 domains that describe important areas of daily living that are affected by treatment for head and neck cancer including pain, appearance, activity, recreation/entertainment, employment, chewing, swallowing, speech, and shoulder disability. Each of the 9 domains has several options within it that allow the patient to describe their current functional status. The highest level or "normal" function is assigned 100 points, whereas the lowest level or greatest dysfunction is scored 0 points. To obtain the final composite score, the scores within each of the 9 QOL domains are summed. Each category contributes equally in the final composite score of the questionnaire of 900 points. The purpose of the questionnaire was explained in detail and informed consent was obtained in accordance with an approved human subject protocol.
Data are summarized as the mean±SD. To assess the influence of the 2 operative modalities on postlaryngectomy QOL, the composite QOL scores of the 2 groups were compared with each other. Significance levels were determined by the student’s t test. We then used a stepwise logistic regression equation to analyze the possible 13 influencing factors of postlaryngectomy QOL including sex, age, living partners, degree of education, styles of communication, chronic diseases before or after operation, cancer stage, types of tumor, operative modality, neck dissection, duration after operation, postoperative radiotherapy or chemotherapy and complications. Statistical analyses were done with the SAS6.12 software.
Results
Comparison of QOL between the two groups
The composite QOL scores of 81 patients treated by partial-laryngectomy were higher than those of the 37 patients treated by total-laryngectomy with a statistically significant difference (692.3 ±127.9 (SD) vs. 636.4±140.0, P<0.05, Table 2). Of the 9 domains comprised in the questionnaire, the scores of speech and appearance were higher in the partial-laryngectomy group compared to the total-laryngectomy group (P<0.001; P<0.05). But the total-laryngectomy group gave higher scores than the partial-laryngectomy group in the domain of pain (P<0.01).
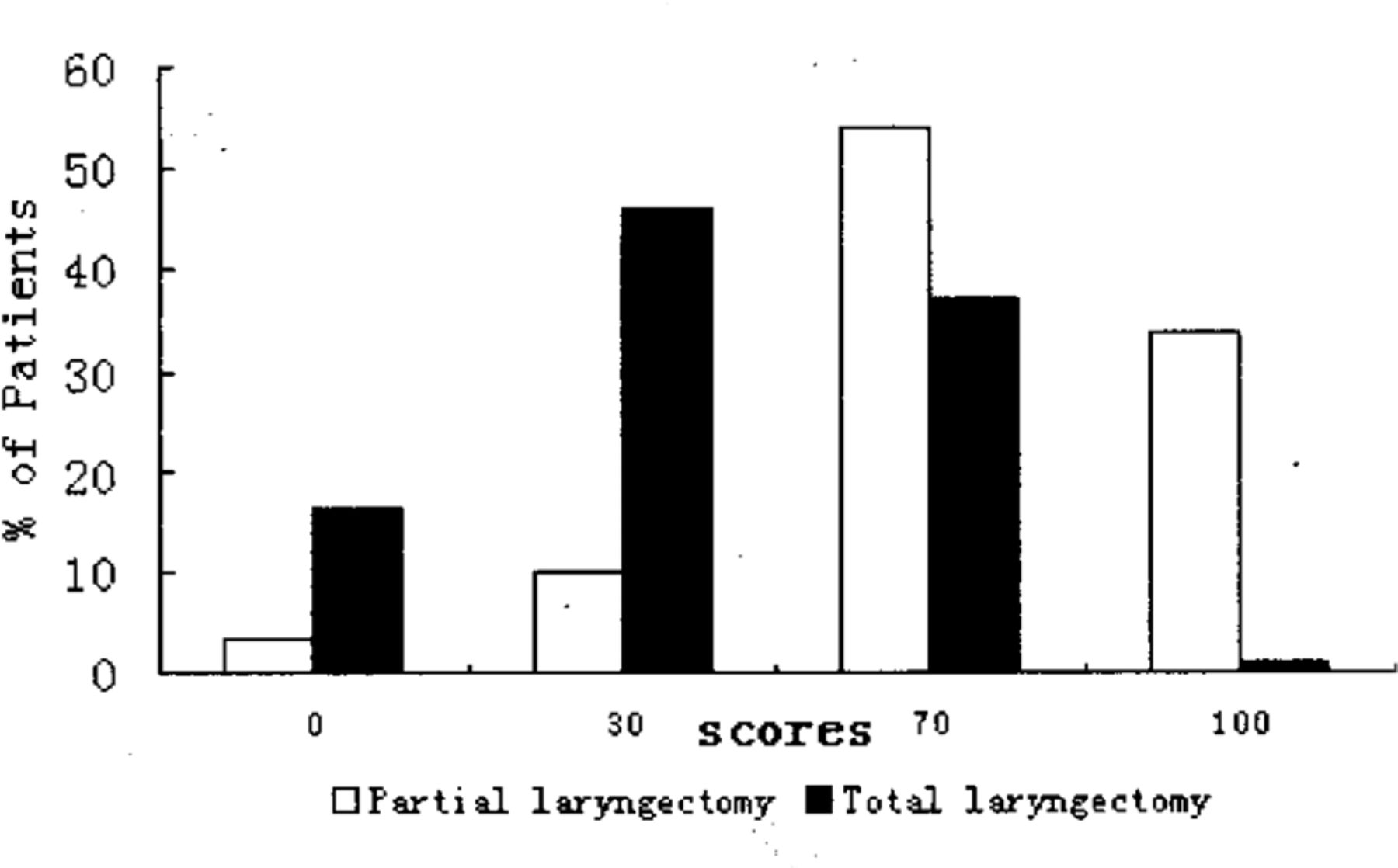
In the responses, 87.7% of the partial-laryngectomy patients chose the items of “My speech is the same as always” (100 points) or “I have difficulty with saying some words, but I can be understood over the phone” (70 points) in the speech domain. These responses were selected by only 37.9% of the patients in the total-laryngectomy group (Fig.1). On the contrary, the patients who chose the items of “Only my family and friends can understand me” (30 points) or “I cannot be understood” (0 points) accounted for 12.4% patients in the partial-laryngectomy group, but 62.3% in the totallaryngectomy group.

Comparison of the partial-laryngectomy group with the total-laryngectomy group in the speech domain.
Whereas 81.5% of the partial-laryngectomy patients chose the items of “There is no change in my appearance” (100 points) or “The change in my appearance is minor” (75 points), only 54.1% of the patients in the total-laryngectomy group chose these 2 items (Fig.2). Almost half of the patients in the total-laryngectomy group chose “My appearance bothers me but I remain active” (50 points).

Comparison of the partial-laryngectomy group with the total-laryngectomy group in the appeamnce domain
Factors influencing postlaryngectomy QOL
Six influencing factors entered the stepwise logistic regression equation at a level of P=0.2 when we set 13 standardized possible influencing factors as independent variables, and set ranked QOL scores of patients as dependent variables (Table 3). According to the OR values, the 6 factors related to postlaryngectomy QOL included cancer stage, operative modality, complications, postoperative radiotherapy or chemotherapy, living partners and chronic disease before or after operation. The QOL of the patients treated with partial laryngectomy was 0.329 of those treated by total laryngectomy (P=0.009). The data suggest that the postoperative QOL of the patients without radiotherapy or chemotherapy, undergoing partial laryngectomy, living with their family, without chronic diseases and complications and with an early stage of cancer was better than those with opposite conditions.
DICUSSION
It is obvious that the head and neck are important sites with many vital functions closely related to normal life, such as speaking, breathing, equilibrium and so on. Malignant tumors and operative treatments lead to dysfunction and disfigurement, and hence to psychosocial problems, which greatly reduce the QOL of the patients. [4,5] Therefore, head and neck cancers have been described as psychologically highly traumatic cancer types.[5] The 5-year survival rate is not enough to evaluate the outcome of treatment. As a result, the QOL research on patients with head and neck cancers has been of increasingly interest.
The term quality of life has been used as both a concept and an instrument of measurement, but there is no commonly accepted definition.[6] Some authors have expressed quality of life as representing the gap between the perceived realities of what one has and what one wants or expects. However, there are some aspects of the QOL at its most fundamental level which are accepted widely: it is both subjective, including the patient’s view; and multidimensional, covering a broad range of areas of the patient’s life; and dynamic as well, changing throughout time and situations.[2]
Postoperative QOL between total and partial-laryngectomy patients
Our study of laryngeal cancer patients shows that, postoperatively, partial laryngectomy is superior to total laryngectomy in overall QOL. Our results showed that the composite QOL scores of the patients treated by partial laryngectomy were higher than those of the patients treated by total laryngectomy (P<0.05, Table 2). In previous reports, the authors took this point of view for granted because of loss of voice and disfigurement caused by total laryngectomy. But for some reasons as follows, it might not be the case. Partial laryngectomy is sometimes followed by some severe and agonizing complications, such as stenosis of the larynx and severe aspiration. Patients have to endure a cannula or nose feeding for a long time period, so QOL is greatly reduced. Besides, Deleyiannis et al.[7] demonstrated using the UW-QOL questionnaire that, in spite of the loss of voice, the dysfunctions caused by a total laryngectomy do not necessarily translate into an overall worse QOL. In addition, some investigations showed that many patients treated by total laryngectomy do not consider speech as their most important QOL feature. To our knowledge, ours is the first report demonstrating, using a QOL questionnaire, that partial laryngectomy is superior to total laryngectomy in overall QOL.
Three of the 9 domains comprised in the UW-QOL questionnaire were significantly different between partial and total-laryngectomy groups (Table 2). One was the speech domain which had the most significant difference of scores between the 2 groups. In this domain, the partial-laryngectomy group showed higher scores than the total-laryngectomy group, in which the score of speech was also the lowest of the 9 domains. This result indicates that speech is the most important aspect influencing overall QOL. Although some methods have been used to recover and reconstruct speech, such as esophageal speech, artificial larynx, electrolaryngeal speech and tracheoesophageal speech and so on, their efficacy and popularization are not satisfying. In our study, 62.3% of the patients treated by total laryngectomy considered that “Only my family and friends can understand me” and “I can’t be understood” which is consistent with what De Boer et al.[8] reported. We also found that many patients treated by total laryngectomy are often in a bad mood and easily get angry when they can not be understood. Therefore, it is the clinicians’ responsibility to try their best to preserve speech of patients with laryngeal cancer, hence to improve their postoperative QOL.
A second domain with a significant difference was appearance. Our study shows that the partial-laryngectomy group had a better view of their appearance than the total-laryngectomy group. This result is supported by a study by De Boer et al.,’[8]’ who reported that 56% of the total-laryngectomy patients considered their appearances was moderately or severely damaged by treatment. The disfigurement caused by total laryngectomy mainly comes from the formation of a tracheal stoma. It is a symbol of deformity. It destroys patients’ social confidence and reduces their interest in showing up in public, hence greatly reduces the QOL.
The final domain with significant difference between the 2 groups was pain. Unexpectedly, our study showed that the patients treated by a total laryngectomy have less pain than those treated by a partial laryngectomy. To a great extent, the pain after treatment is related to the treatment modality itself. Pain induced by chemotherapy could impair the psychological health more than other complications such as dysphagia. Some studies showed that the patients had less pain after operation than after chemotherapy alone,[4,7,9] and loss of innervations might explain this phenomenon. [4,9] However, until now, the difference of pain between operative modalities has not been reported. One possible reason for less pain after total laryngectomy is that more sensory nerves from the skin and mucous membranes are cut off compared to partial laryngectomy. A further study is required to elucidate the underlying mechanism.
Influencing factors of postlaryngectomy QOL of the laryngeal cancer patients
Besides operative modalities that can influence the postlaryngectomy QOL of these patients as mentioned above, we also analyzed other possible influencing factors, so as to predict postoperative QOL of patients, set up a suitable rehabilitation plan and speed physical and psychological recovery. Our study shows that 6 factors including stage of the cancer, operative modality, complications, postoperative radiotherapy or chemotherapy, living partners and chronic diseases before or after operation are related to postlaryngectomy QOL (Table 3). The results suggest that clinicians should try to make an accurate diagnosis and provide earlier treatments, improve their operative skills and emphasize postoperative nursing. In so doing it will help to avoid complications, and lessen pain and other suffering from radiotherapy and chemotherapy. Moreover, more encouragement and understanding from families and society should be given to these patients after operation to provide a normal life as soon as possible. Especially, the majority of laryngeal cancer patients are middle-aged and old men, who are subject to many chronic diseases such as diabetes mellitus or chronic bronchitis. These chronic diseases are a heavy burden on the patients and their families both economically and psychologically, so society should give them and their family more material and psychological support.
Concerns about the application of the UW-QOL questionnaire in China
At present, many special QOL questionnaires regarding head and neck cancers have been used, but none of them have been unanimously accepted. Our study shows that, as a whole, the UW-QOL questionnaire is a good QOL instrument for QOL studies of laryngeal cancer patients in China based on the following reasons. The UW-QOL questionnaire is short and comprehensible, including most important aspects of interest, and it has proved to have relatively high validity and reliability by many investigations. In our study, the questionnaire distinguished the QOL differences between the 2 groups showing its validity and responsiveness. In addition, 91% of the follow-up letters were sent back, with almost all of the questionnaires being suitable and qualified for analysis. Moreover, developing new QOL or health-status measures is a time-consuming, expensive, and painstaking process, requiring years of research, instrument testing, and validation.[10] Therefore, our study suggests that investigators should use an existing instrument rather than develop and validate a new one, and that the UW-QOL questionnaire is suitable for studies of laiyngeal cancer.
In conclusion, this study shows that partial laryngectomy is superior to total laryngectomy in overall postoperative QOL, Three of 9 domains comprised in the UW-QOL questionnaire, consisting of speech, appearance and pain, are significantly different between partial and total-laryngectomy groups. Besides operative modality, cancer stage, complications, postoperative radiotherapy or chemotherapy, living partners and chronic diseases before or after operation are related to postlaryngectomy QOL. As a whole, the UW-QOL questionnaire is a good instrument for studying QOL of laryngeal cancer patients in China, and it can be used to explore the QOL outcome obtained from different reconstructive techniques.
- Received January 20, 2006.
- Accepted March 13, 2006.
- Copyright © 2006 by Tianjin Medical University Cancer Institute & Hospital and Springer
In this issue






{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.