

keywords
Introduction
Choroid plexus papilloma (CPP) is a relatively rare, slow-growing benign tumor (WHO level I). Recently, an adult patient with fourth ventricle choroid plexus papilloma received surgery via a suboccipital midline approach in our hospital. It has been rare in clinical practice to see postoperative hemorrhage occurring in the same patient 3 times. The causes of the hemorrhage were analyzed based on literature regarding postoperative hemorrhage in choroid plexus papilloma and in intracranial tumors. The case involved in our study is described and detailed in the following.
Case Report
A 57-year-old female patient was admitted to Northern Jiangsu Province People’s Hospital due to frequent headaches for 1 week. Physical examination showed that the patient was conscious, clear in speech, a little slow to react, and had round, symmetrical pupils (3 mm) with equal reaction to light. There was no edema in the optic papilla, no resistance reflex in the neck, and the finger-to-nose test with alternating movement, Romberg’s sign and bilateral Babinski test were all negative. Head CT scan showed that the lesion was located in fourth ventricle and near the cerebellar midline. CTA of the head proved that the tumor blood supply came from both sides of the posterior inferior cerebellar artery. MRI revealed a tumor with slightly longer signal on the TIWI image and a longer signal on the T2W1 image in the enlarged fourth ventricle; the lesion was clearly enhanced after injection of contrast agent (Fig. 1). Coagulation before surgery was normal. After careful preoperative preparation, tumor resection through a suboccipital midline approach was performed under general anesthesia. The surgery was successful, and the tumor was completely resected. Postoperative pathologic examination showed that the tumor was a choroid plexus papilloma (Fig. 2). Head CT scanned 23 h after surgery showed no fresh hemorrhage in the surgical site (Fig. 3).

MRI revealed a tumor with slightly longer signal in the TIWI image and a longer signal in the T2W1 image in the enlarged fourth ventricle; the lesion was clearly enhanced after injection of contrast agent.
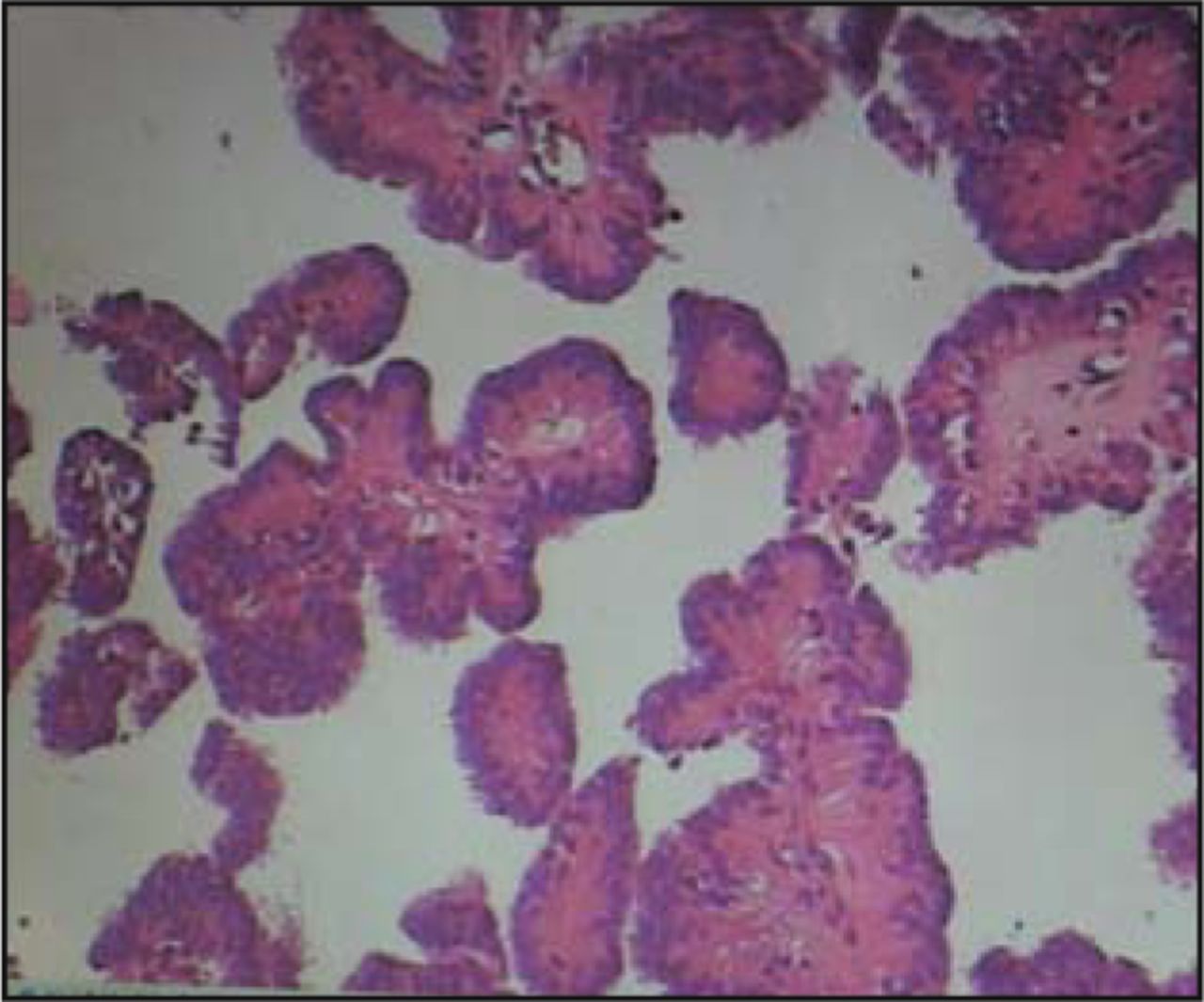
Postoperative pathologic examination showed the tumor was a choroid plexus papilloma.

Head CT scanned 23 h after surgery showed no fresh hemorrhage at the surgical site.
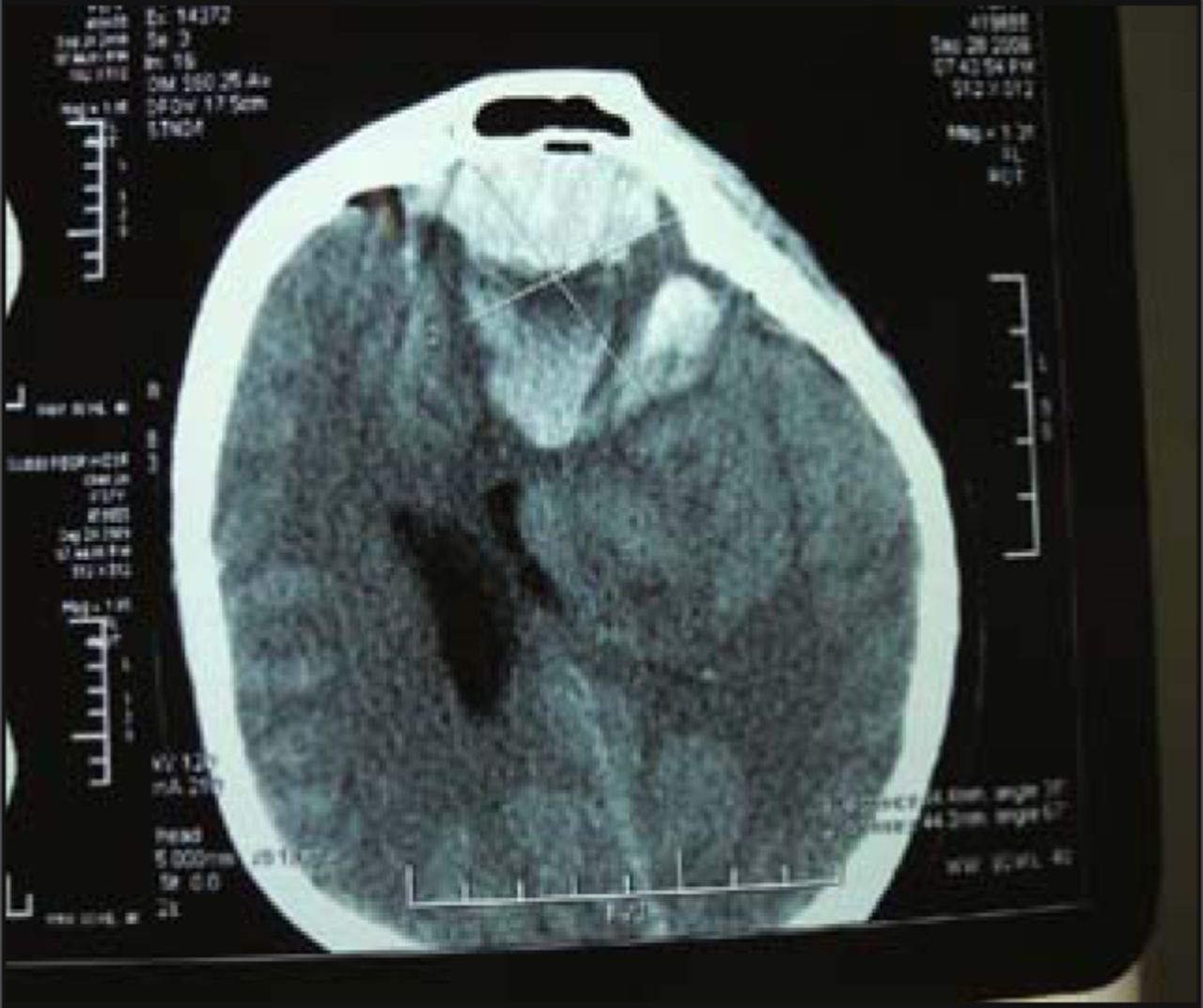
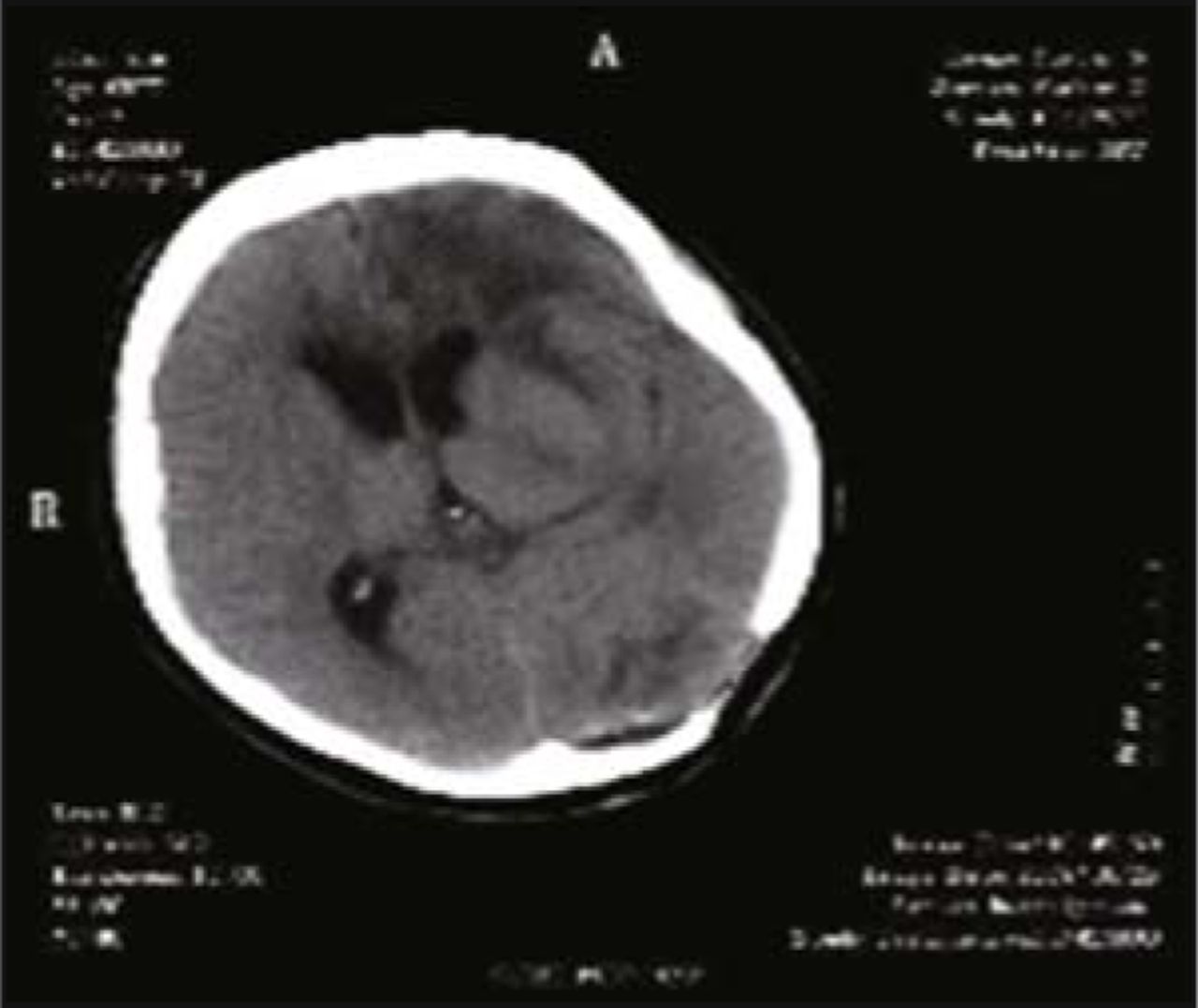
Altered mental status, however, suddenly occurred in the patient 56 h after surgery; therefore, a repeat head CT scan was performed and showed a left frontal intracerebral hemorrhage with a bleeding volume at about 60ml (Fig. 4). Emergency surgery under general anesthesia was performed immediately to eliminate the hematoma. During surgery under the microscope, we found vascular occlusions that occurred in 3 frontal bridging veins after bleeding along midline near the left frontal area, and we blocked those with electrocoagulation. The operation was successful. After surgery, 1.5 units of erythrocyte supernatant and 200 ml plasma were given to the patient via intravenous infusion. A repeat CT scan of the head was performed 10 h after the second surgery and revealed a hematoma around 35 ml in the left posterior fossa (Fig. 5). Stat testing for coagulation function showed the following: PT (prothrombin time) 17.9 s, VWF (von Willebrand factor) 248%, PT-INR (prothrombin normalized ratio) 1.46, and D-dimers 12.73 μg/ml. These parameters were higher than standard levels. FIB (fibrinogen) was 1.34 g/L which was lower than normal. Again, a third surgery with the purpose of removing the hematoma was immediately performed under general anesthesia. The patient was transfused with 300 ml plasma and 1.0 unit of fibrinogen postoperatively. After 3 surgeries, the patient was persistently comatose, and repeat head CT scan showed no further hemorrhage in the brain (Fig. 6). As the patient was running a fever during the course of disease, she was treated for inflammation, given supplemental nutrients for nerve repair, given medication to arouse her brain as well as prophylaxis for gastric stress ulceration. After treatment, the patient’s consciousness gradually improved and her temperature returned to normal. One month after the last operation, the patient had a large amount of fresh bloody stool on 2 occasions which failed to resolve with conventional hemostatic therapy. DSA of both sides of the internal iliac artery angiography showed that the peripheral blood vessels of the inferior rectal artery in the right side were clearly disordered (Fig. 7). The feature of contrast agent overflowing and a small hemangioma at the end of the right inferior rectal artery were also seen by angiography. By way of DSA, arterial embolization was performed in which the blood vessels in the lesions were embolized (Fig. 8). As a result, the patient’s bloody stools were completely controlled. In the following days, the patient was treated with anti-inflammatory drugs and given nutritive support. Consequently, she gradually got better, regained consciousness and resumed regular sleeping and eating. When discharged from the hospital the patient’s functioning in her limbs was good, but her speech was not fluent.

Repeated CT scan performed 56 h after surgery showed left frontal intracerebral hemorrhage.

Repeat head CT 10 h after the second operation revealed a hematoma approximately 35 ml in the left posterior fossa.

CT scan performed before the patient was discharged.

DSA of both sides of the internal iliac artery angiography showed obvious disorder in the peripheral vascular of the inferior rectal artery on the right side.
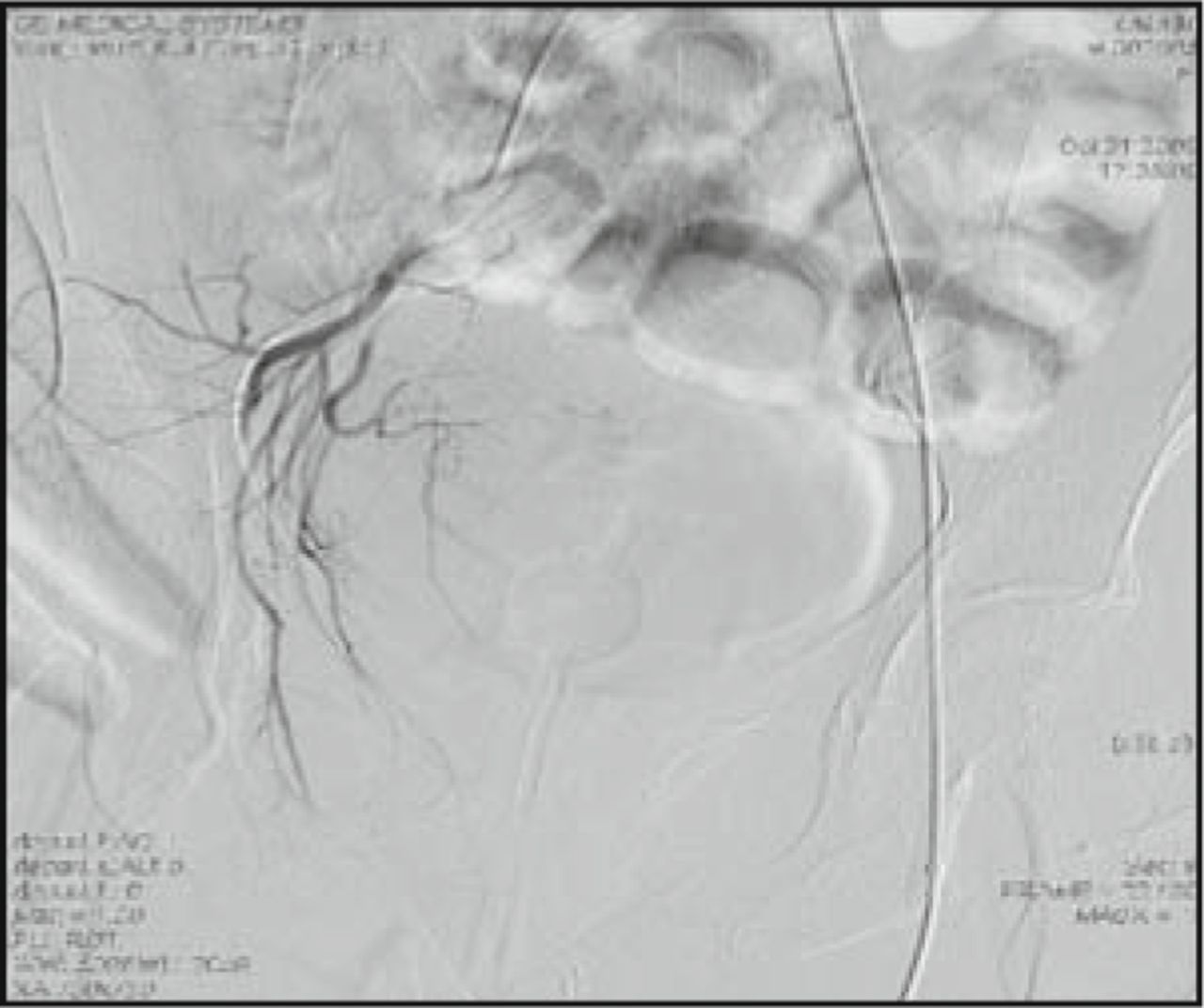
Arterial embolization was performed in which the blood vessels in the lesions were embolized.
Discussion
Choroid plexus papilloma is a type of epithelial tumor originating from the choroid plexus of the ventricles. It has been reported in the literature[1,2] that choroid plexus papillomas account for about 0.4%-0.6% of the total number of intracranial tumors. CPPs commonly occur in the triangular area of the lateral ventricle supratentorially in children and infants, while they commonly occur in the fourth ventricle subtentorially in adults and adolescents. The typical signs and symptoms often associated with hydrocephalus caused by intracranial hypertension, include headache, nausea, vomiting, ataxia, and retardation. CT scan of the head usually shows an intraventricular identical to high-density space-occupying lesion which can be enhanced by contrast agent. Hydrocephalus is commonly seen in CPP, and it may be caused by an obstruction in the ventricular outlet, by tumors producing excessive cerebrospinal fluid, spontaneous tumor hemorrhage or tumors secreting protein-like substances in the cerebrospinal fluid which deposits in the subarachnoid space, arachnoid villi and arachnoid granulations[3]. MRI generally has identical to low signal in TIWI imaging and a high signal in T2W1 imaging; contrast enhancement is apparent[4]. Surgery is the primary way to treat choroid plexus papilloma, and it can totally remove the tumor, resulting in the best treatment outcome. The tumor may be cured in this way. It has been reported in the literature[4] that the 5-year survival rate of CPP patients has reached up to 100%. Choroid plexus papilloma of the fourth ventricle are typically located near the central hole of the middle lower part of the fourth ventricle, and the suboccipital midline approach is often employed in surgery. Choroid plexus papilloma is a type of vascular-rich tumor, and the blood supply to tumors in the fourth ventricle is mainly from the posterior inferior cerebellar artery. To deal with this tumor, we should first cut off the tumor blood vessel pedicle, and then remove this tumor totally in order to avoid uncontrollable bleeding caused by the block resection.
This patient developed postoperative hemorrhage 3 times. The first 2 times included intracerebral hemorrhage and epidural hemorrhage. There are no positive conclusions about the mechanism of postoperative intracranial hematoma outside of the surgical site. The causes of bleeding in this patient were mainly associated with the following factors.
i) Altered intracranial pressure: utilization of dehydrating agents or overdrainage from the residual cavity of the removed tumor results in a sharp decrease in intracranial pressure over a short time, and consequently, distant blood vessels retract and may break, causing bleeding. Excessive decompression after the resection of intracranial tumors and overdrainage of cerebrospinal fluid alter the balance of intracranial dynamics, and brain tissue collapses and shifts, resulting in the rupture of bridging veins of the cerebral cortex and subsequent hemorrhage[5,6]. In this case, the cause of the first intracerebral hemorrhage far away from the area of the removed tumor was due mostly to this reason. In addition, many small blood vessels from the dura mater supplying blood to the skull, the derivative veins of the superior sagittal sinus, and the abnormal middle meningeal arterial branches can cause the epidural bleeding[7]. When lesions are removed, the intracranial environment becomes imbalanced due to the reduced brain volume, and an acute or chronic decrease in intracranial pressure leads to the pulling of the brain by its own weight; therefore, it makes the epidural space lose support, resulting in the separation of the dura mater and the inner periosteum of the skull. Consequently, the above vasculature may rupture and lead to bleeding[8]. These factors may have led to the patient’s second epidural hemorrhage.
ii) Surgery can result in damage to endothelial cells of the cerebral vasculature, and releasing thromboplastin into the blood can activate the coagulation system, while at the same time, releasing vasoactive peptides from the hypothalamus induce coagulation dysfunction[7,9]. Component blood transfusion is given intraoperatively or postoperatively due to low levels of clotting factors in the blood, reduced platelet survival, and due to the presence of anticoagulants in the blood. Although they do not directly cause bleeding, they are underlying factors that result in massive bleeding. This could explain the phenomenon in our patient that while preoperative coagulation function was normal, repeated tests on coagulation function became abnormal after the second intracranial hemorrhage.
iii) In addition, in order to prevent accidents such as apnea or foreign body aspiration, this patient went back to the wards from the OR after surgery with tracheal intubation. Awake from anesthesia, the patient had high blood pressure induced by a variety of factors, such as intubation stimulation, restlessness, severe coughing during extubation, and these factors may also cause cerebral blood vessel rupture and hemorrhage[7]. These factors were not excluded in our case.
The third episode of hemorrhage in this patient was caused by the rupture and bleeding from small branches of the inferior rectal artery. Rattunde et al.[10] have reported 1 case where postoperative cerebral hemorrhage developed, accompanied by a large amount of bloody stool after surgery, where examination revealed that the inferior rectal artery caused bleeding which was stopped after embolization. The relationship between cerebral hemorrhage and bleeding at the inferior rectal artery, or in other words the relationship between choroid plexus papilloma and the inferior rectal artery bleeding is still inconclusive. However, in course with poor peristalsis, the symptoms of constipation are aggravated in patients with a past history of constipation and hemorrhoids who have been confined to bed. The inferior rectal arteries in females are localized to the lower segment of rectum and vagina, and bleeding can be caused by constipation and dry stool.
Conflict of interest statement
No potential conflicts of interest were disclosed.
- Received January 7, 2010.
- Accepted February 10, 2010.
- Copyright © 2010 by Tianjin Medical University Cancer Institute & Hospital and Springer
In this issue






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.