

Abstract
OBJECTIVE To observe and evaluate the value of utilizing selective internal iliac artery infusion and selective internal iliac artery embolization for the treatment of unremitting gross hematuria of stage T4 bladder carcinoma.
METHODS Fifty-eight stage T4 bladder carcinoma patients were selected. The patients were grouped to the TAI group and the TAE group. The main symptom of hemorrhage was gross hematuria. None of the patients in our study could receive trunk embolization. The infusion plan was oxaliplatin (100 mg/m2) and epirubicin (EPI 50mg/m2). Embolization was done with coils or strips of gelatin sponge. The duration of gross hematuria was observed. Routine urinalysis and routine blood examination were performed. EORTC QLQ-C30 was used to evaluate the quality of life before and aft er treatment.
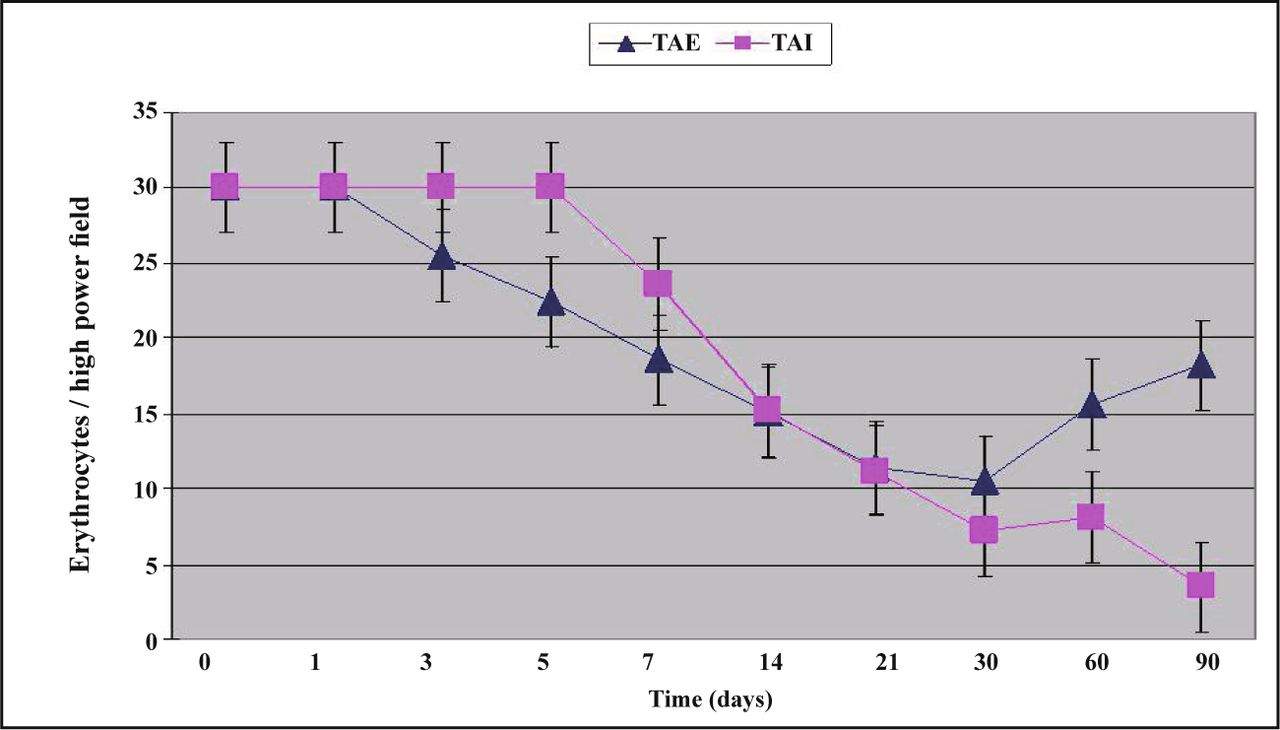
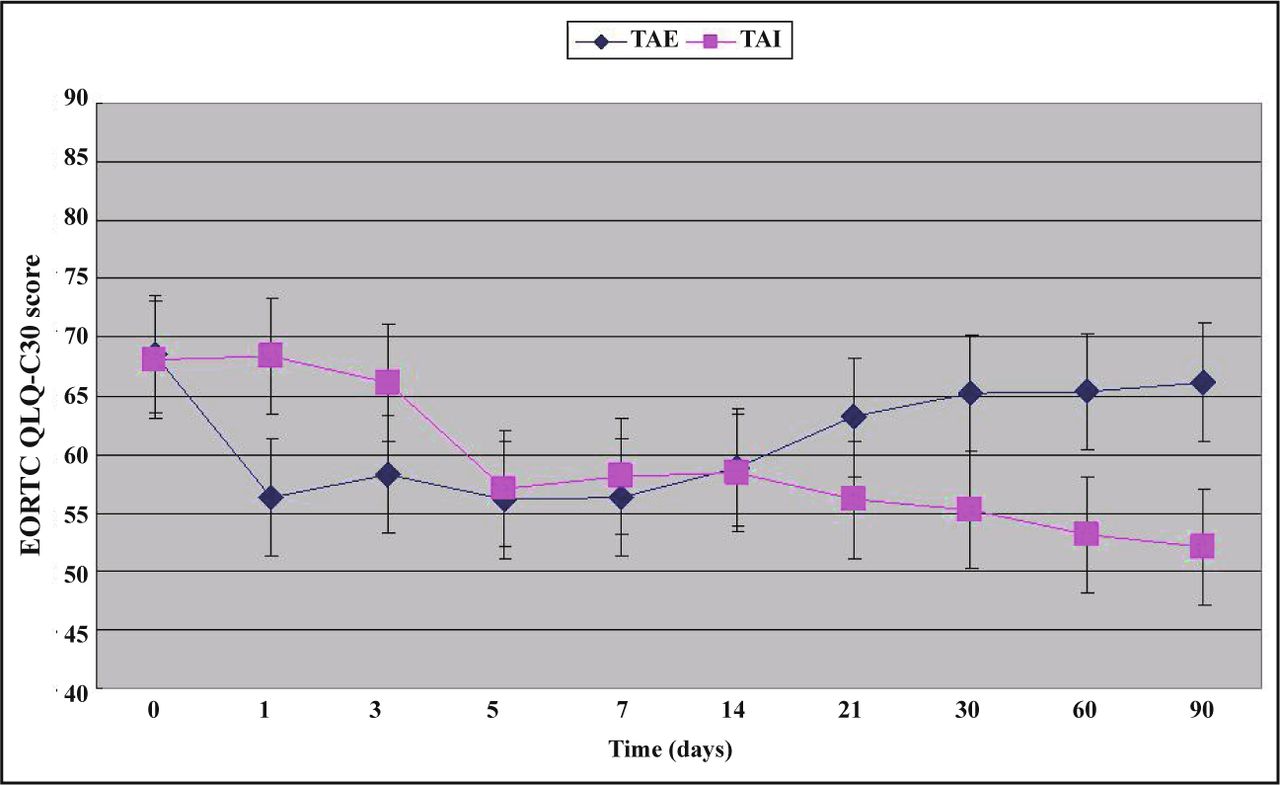
RESULTS Gross hematuria and hematuria by light microscope in all patients were reviewed. Resolution time of gross hematuria in the TAI group was 6.7 ± 1.8 days and that in the TAE group was 3.5 ± 0.7 days. The changes in routine urianlysis, routine blood examination and EORTC QLQ-C30 are shown in Figs. 1-3. Gross hematuria disappeared in both groups within 7 days aft er treatment, but the time for the gross hematuria to resolve in the TAE group was much less than that in TAI group (t = 2.51, P < 0.01), and there were no significant differences in the 7th and 21st day between the 2 groups. On the 90th day, the number of erythrocytes in the urine was near 30, close to gross hematuria. The EORTC QLQ-C30 scores decreased after interventional therapy in both groups, which means that quality of life was increased, but there were no significant differences between the 2 groups.
CONCLUSION Selective internal iliac artery infusion and selective internal iliac artery embolization are safe, and, in our study, therapeutic efficacy was satisfactory in treating unremitt ing gross hematuria of stage T4 bladder carcinoma in patients who could not receive trunk embolization. TAE can stop gross hematuria in the short term, but it can be used just once and the long-term therapeutic effect is not satisfactory. TAI had a therapeutic effect similar to TAE, but for a shorter duration, and TAI can be performed multiple times. TAI is one of the facultative treatments for treating gross hematuria of stage T4 bladder carcinoma.
keywords
- selective internal iliac artery infusion
- selective internal iliac artery embolization
- hematuria
- stage T4 bladder carcinoma
- oxaliplatin
Introduction
Gross hematuria is one of the most common symptoms of stage T4 bladder carcinoma[1], which can worsen patients’ general condition[2] and quality of life[3]. It is important to reduce hematuria in the short term in clinical practice[4], but satisfactory hemostasis is difficult to achieve in stage T4 bladder carcinoma patients[5]. Moreover, it is hard for stage T4 bladder carcinoma patients to undergo surgical procedures because of hematuria. Selective internal iliac artery chemoembolization (SII-ACE) or selective internal iliac artery embolization (SI-IAE) is considered first-choice interventional therapy to treat hemorrhage in stage T4 bladder carcinoma[4], but in our clinical practice, many stage T4 bladder carcinoma patients cannot receive selective embolization, which becomes a block in the treatment. Selective internal iliac artery chemotherapeutic infusion may be another facultative technique. However, there is seldom clinical research or comparative studies between embolization and chemotherapeutic infusions. So we designed a retrospective study to observe and evaluate the value of utilizing selective internal iliac artery infusion and selective internal iliac artery embolization for treating gross hematuria of stage T4 bladder carcinoma.
Materials and Methods
General data
This retrospective study was approved by the institutional review board of our hospital; informed consent was waived. From March 2003 to August 2008, stage T4 bladder carcinoma patients with unremitting hematuria for over 7 days were selected for our study. Their main symptom was gross hematuria where good hemostasis had not achieved. Patients with disturbances in blood coagulation, heart function or pulmonary dysfunction were excluded. There were 58 cases with stage T4 bladder carcinoma chosen, among which 46 cases were male and 12 female, and the patients were from 34 to 85 years in age, with a mean age of 64.2 years. The patients would receive either selective internal iliac artery infusion or trunk embolization in our department. Twenty-two cases had a recurrence or metastasis postoperatively, and 30 cases were deemed inoperable when a diagnosis was made; 6 cases deemed inoperable after exploratory laparoscopy; 36 cases deemed inoperable when stage T4 bladder carcinoma diagnosis was made. Fifty-one cases were transitional cell carcinoma; 5 cases adenocarcinoma, and 2 cases were squamous carcinoma. The patients who had an evident internal pudendal artery upon internal iliac arteriography were assigned to group TAE. The patients who had no evident internal pudendal artery were assigned to group TAI. There were 30 cases in group TAI who received selective internal iliac artery infusion, and there were 28 cases in group TAE who received selective internal iliac artery trunk embolization.
Interventional procedure
A catheter was placed in the celiac artery through a femoral arteriopuncture by Seldinger’s technique. Angiography was performed to identify the size, position, type of tumor, presence of possible arteriovenous fistulas and condition of the major arteries. After infusion, the catheter was withdrawn. To avoid bleeding, a pressure dressing was given and patients were kept prone for 24 h.
Group TAI treatment plan
Oxaliplatin (100 mg/m2) and epirubicin (EPI 50 mg/m2) were infused in the iliac arteries bilaterally, and the proportion was according to angiography. If using the iliac artery on one side was more advantageous, then 2/3 of the chemotherapeutic agents would be infused to that side, and the drug would be infused equally when there was no difference between the 2 sides. The regimen was repeated every 4 weeks. Group TAI received a total of 3 cycles of treatment.
Group TAE treatment plan
Embolization was done with coils when the catheter was sent selectively into the internal iliac arterial trunk. The diameters of the coils was 8 mm, and length was 5 cm. Strips of gelatin sponge were used when necessary, and arteriography was used to check the effect of embolization. All of the patients received 1 cycle of treatment.
Follow up and valuation standard
All the patients were followed up for 3 months. The duration of gross hematuria was observed. Routine urianlysis and routine blood examination were performed. EORTC QLQ-C30[6] was used to evaluate the quality of life before and after treatment.
Duration of gross hematuria
Duration of gross hematuria was observed after treatment, and assessed mainly by the extinction time of gross hematuria.
Routine urinalysis
Routine urinalysis was made on the 1st, 3rd, 5th, 14th, 21st, 30th, 60th, 90th day after treatment. The number of erythrocyte were counted in 3 high power fields microscopically, and the mean was utilized as the result. If there were too many erythrocytes, a count of 30 was used.
Routine blood examination
Routine blood examination was done on the 1st, 3rd, 5th, 14th, 21st, 30th, 60th, 90th day after treatment to evaluate hemoglobin.
Quality of life
EORTC QLQ-C30 (version 3.0) was used to evaluate the quality of life before and after treatment.
Statistical analysis
Statistical treatment of the data was made using statistics software (SSPS, version 11.0), and was considered significant P < 0.05.
Results
Bilateralis internal iliac arteriography was carried out before arterial perfusion or embolization. None of the tumors stained in 7 cases (12.07%). There was obvious tumor stain in 51 cases (87.93%) with bilateralis blood-supply in 39 cases (67.24%) and single blood-supply in 12 cases (20.69%). No death occurred during treatment or during follow-up. The most frequent side effects in group TAI were nausea, vomiting, and lassitude due to the chemotherapeutics, while those in group TAE were pain and fever due to tumor ischemia and necrosis.
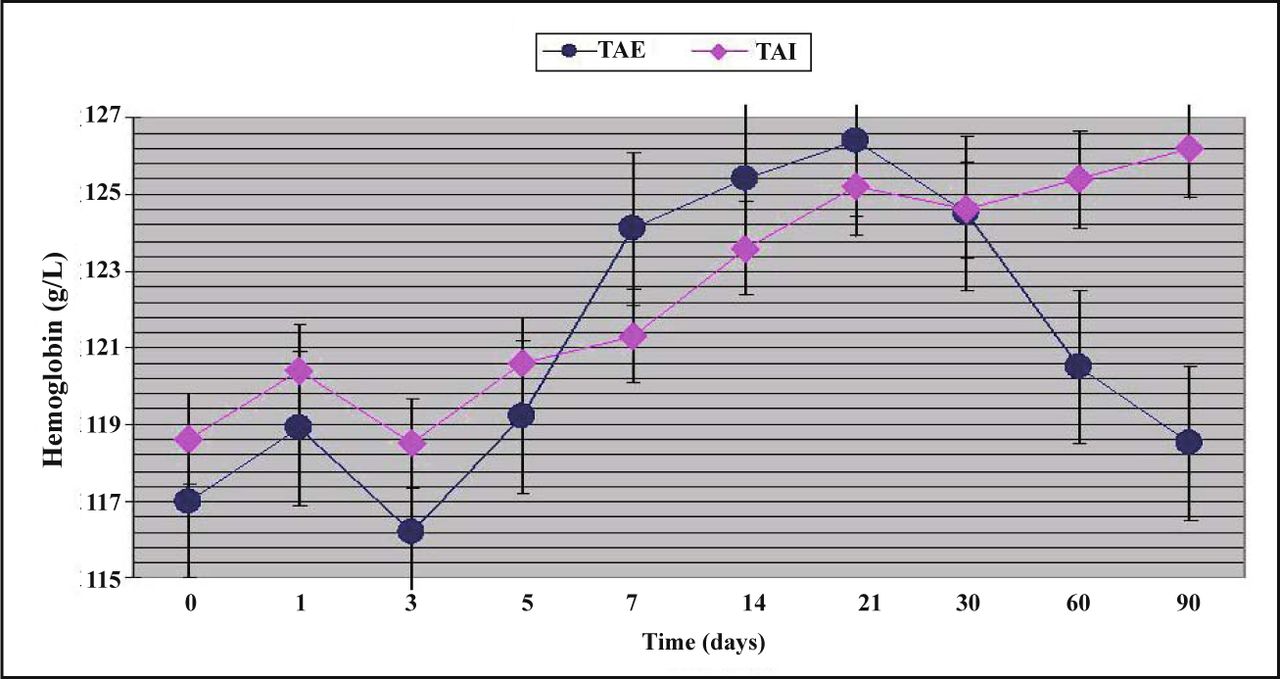
Gross hematuria and microscopic hematuria were performed in all patients. For changes in hemoglobin, see Fig. 1, and for changes in urine erythrocytes, see Fig. 2; for changes of EORTC QLQ-C30, see Fig. 3. Resolution time of gross hematuria in the TAI group was 6.7 ± 1.8 days and that in the TAE group was 3.5 ± 0.7 days. The changes in routine urinalysis, routine blood examination and EORTC QLQ-C30 are shown in Figs. 1-3.

Changes in hemoglobin.

Changes in urine erythrocytes.
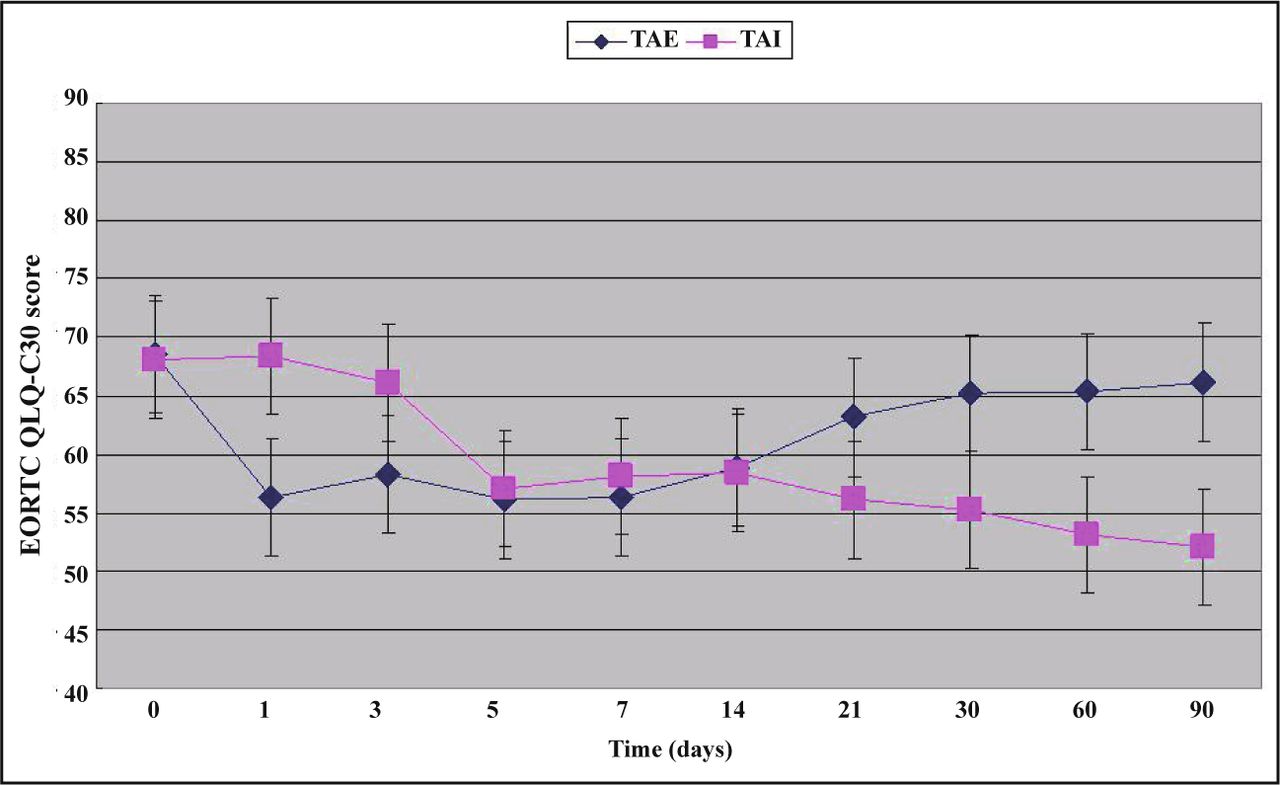
Changes in EORTC QLQ-C30.
Gross hematuria disappeared in both groups within 7 days after treatment, but the time for the gross hematuria to resolve in the TAE group was much less than that in the TAI group (t = 2.51, P < 0.01), and there were no significant differences in the 7th and 21st day between the 2 groups. On the 90th day, the number of erythrocytes in the urine was near 30, close to gross hematuria. The EORTC QLQ-C30 scores decreased after interventional therapy in both groups, which means that quality of life was increased, but there were no significant differences between the 2 groups.
Discussion
Persistent and intermittent gross hematuria is the most frequent, almost the exclusive symptom, of stage T4 bladder carcinoma[7]. Gross hematuria brings physiological and psychological stress to patients which decreases patient compliance and even influences prognosis[8]. Neovasculature and blood vessel dysplasia are characteristic of malignant tumors[9]. Malignant tumors show affluent blood supply in arteriography (Fig. 4). Invasion into vessels and into the mucous membrane of the urinary bladder is a cause of hematuria in stage T4 bladder carcinoma patients[10] (Fig. 5). Anomalous vessel structure and disturbances in blood coagulation lead to unsatisfactory therapeutic hemostasis[4]. Chemotherapy, radiotherapy and irrigation of the bladder is cytotoxic to cancer cells and leads to hematuria[11]. However, low drug levels, locally and myelosuppression limit the need for hemostatic drug agents[6].

Black arrow shows the mass intruding into the urinary bladder on pelvic CT scan.

Black arrow shows tumor stained on internal iliac arteriography.
Interventional therapy is an important treatment for the alleviation of symptoms in stage T4 bladder carcinoma and includes embolization and infusion. Embolization of the terminal branch is difficult to do because the feeding artery of stage T4 bladder carcinoma is seldom found. Coils were used to embolize the main branch of the feeding artery[12], and microparticles were used to embolize the terminal branch[13]. Embolization of the main branch of feeding artery was usually performed in cases of emergency bleeding[14]. But embolization of the main branch has poor repeatability, even when performed just once.
There are some characteristic features of selective internal iliac artery infusion[15]. Firstly, arterial infusion leads to high drug concentrations locally in tissue, including in the urinary bladder and in lymphoid tissue. It has been reported that local tissue has more than 200 to 400 times the drug concentration after selective internal iliac artery infusion, compared to that of intravenous chemotherapy, and the drug concentration in tumor tissue has 5-20 times of that in normal tissue. Secondly, some concentration dependent chemotherapeutics, such as adriamycin can act on DNA of tumor cells directly and have more than 2 to 20 times of the drug concentration via arterial infusion in comparison to that via intravenous chemotherapy[16]. Because of the first pass effect, chemotherapeutics concentrate in bladder tumors with a lower concentration than in other organs. So, interventional infusion has less influence on the heart, brain and kidney.
Cisplatin or carboplatin with epirubicin was considered the classic regimen in treating stage T4 bladder carcinoma, but the administration of cisplatin or carboplatin was limited due to their serious gastrointestinal effects and renal toxicity[17,18]. Oxaliplatin had characteristics of better therapeutic effect, poorer gastrointestinal tract effects and less drug resistance compared with other platonic drugs[17,18]. However, oxaliplatin was seldom used in interventional infusions. EPI is a kind of anthracene nucleus chemotherapeutic with strong cellular intravasation[19]. Internal iliac artery infusion with oxaliplatin and EPI can help control recurrence, metastasis and progression, and even increase in life span [20].
In our research, all of the cases were diagnosed as stage T4 bladder carcinoma. In the TAI group, there was no myelosuppression, hepatic or renal toxicity. It may be that local infusion had lower dosages than intravenous chemotherapy. Further, the duration of hematuria was much less in the TAE group than that in the TAI group (P < 0.01), which showed that TAE would be appropriate for hemostasis in the short term. Erythrocytes in urine, hemoglobin and quality of life on the 7th, 14th, 21st, 30th, 60th day demonstrated that TAI had effects similar to TAE, but that TAI had better results than TAE on the 90th day. So we think that TAI is appropriate for long term treatment. It was reported that collateral circulation can form within 24 h after embolization[21]. Perhaps this can explain the reason why erythrocytes in the urine has a tendency to increase in the TAE group. Though the time to resolution of gross hematuria in the TAI group was longer than that in the TAE group, the therapeutic efficacy was similar between the 2 groups. It should be pointed out that the correlation between the number of infusions and therapeutic effect deserves further research.
In our study, the EORTC QLQ-C30 scores of the 2 groups decreased, and the quality of life was increased. The reason maybe as follows: immunosuppressive therapy was stopped after treatment, and the nutrients consumed by the malignant tissue were decreased. However, we think that the most important reason is that the gross hematuria disappeared in 7 days in both groups, which alleviated mental stress in patients and improved their quality of life.
In a word, selective internal iliac artery infusion and selective internal iliac artery embolization are effective in treating gross hematuria of stage T4 bladder carcinoma in patients who cannot receive trunk embolization. TAE can stop gross hematuria in the short term. However, it can be used just once, and the long-term therapeutic effect is not satisfactory. TAI has a therapeutic effect similar to TAE for a period of time longer than TAI, and TAI can be performed multiple times. TAI is one of the facultative treatments for gross hematuria in stage T4 bladder carcinoma.
Conflict of interest statement
No potential conflicts of interest were disclosed.
Footnotes
This work was supported by the China National Science & Technology Pillar Program during the Eleventh Five-year Plan Period (No. 2007BAI05B06).
- Received December 23, 2009.
- Accepted February 12, 2010.
- Copyright © 2010 by Tianjin Medical University Cancer Institute & Hospital and Springer
References
In this issue






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.