

Abstract
Gastrointestinal duplication is an uncommon congenital abnormality, and colonic duplication combined with teratoma has rarely been reported. A 24-year-old man presented to the Emergency Department with a sudden onset of severe abdominal pain lasting 2 hours without intermission, and also complained to have who had chronic constipation since his birth. Multislice CT imaging showed 2 masses in the retroperitoneal space. The one huge cystic mass was detected behind the transverse colon, pancrease and stomach without infiltration into the surrounding tissues. The right mass containing soft tissues and bones pushed aside the inferior vena cava and right kidney. The cystic duplication and the right mass were excised separately. This case indicates that a patient diagnosed as colonic duplication should receive further differential diagnosis to identify if it coexists other diseases, especially the teratoma.
keywords
Introduction
Gastrointestinal duplication is mostly located in the small-bowel tract and is an uncommon disease, presenting symptoms like abdominal pain, bleeding, obstruction and even perforation[1-5]. The mature teratoma is a benign neoplasm that comes from pluripotential cells of embryonic remnants of the ectodermal lines, which consist of cystic and solid elements including teeth, hair, cartilage and dermal appendages, such as hair follicles and sebaceous material[6,7].
Case Report
A 24-year-old man presented to the Emergency Department of the Affiliated Hospital of Medical College of Chinese People’s Armed Police Forces, Tianjin, with a sudden onset of severe abdominal pain lasting 2 hours without intermission and chronic constipation, which presented since he was born. The abdominal examination showed upper abdominal tenderness, abdominal muscle rigidity and rebound tenderness. Blood samples revealed that WBC was 6.7 × 109/L, with NEUT 81.0%, and the results of the other blood tests and urine test were all in normal ranges. Ultrasonography demonstrated 2 well-defined complex masses in the upper retroperitoneal region. The obvious calcification and fat fluid level were detected within the wall of the right mass, and the left mass looked like a cyst, which showed a high degree of reflection and shadowing in the ultrasonography (Fig.1A). Computed tomography (CT) revealed a twisted huge cystic mass (14.1 cm × 13.0 cm × 9.7 cm) behind the transverse colon, pancrease and stomach, which pressed the pancrease becoming thinner and flat, and another mass (7.9 cm × 7.2 cm × 5.1 cm) was found in the area of the right adrenal gland, which showed shadow of fat and calcification on CT scan (Fig.1B). During the exploratory operation, the fibrous tissue covering the cystic mass and adhering to pancrease and stomach was dissociated, and then the round, twisted mass was exposed, which was swollen in the middle part of the mass and thin in 2 ends of the mass. The right side of the mass pushed aside inferior vena cava and right kidney adhering to the common bile duct. The total tumors were successfully removed in the surgery (Fig.2). Pathological report showed that the left mass was as long as 36 cm and varied from 2.5cm to 4cm in width; the thickness of the cystic wall varied from 4 mm to 8 mm; and the cyst contained muscle and colonic mucosa layer with accumulated lymphocyte nests which was built by the infiltrated lymphocytes, and it was diagnosed as colonic duplication. Teratoma was diagnosed because another mass in the right cavity comprised of fat, bone and cartilage. Pathological examination revealed no evidence of malignancy.
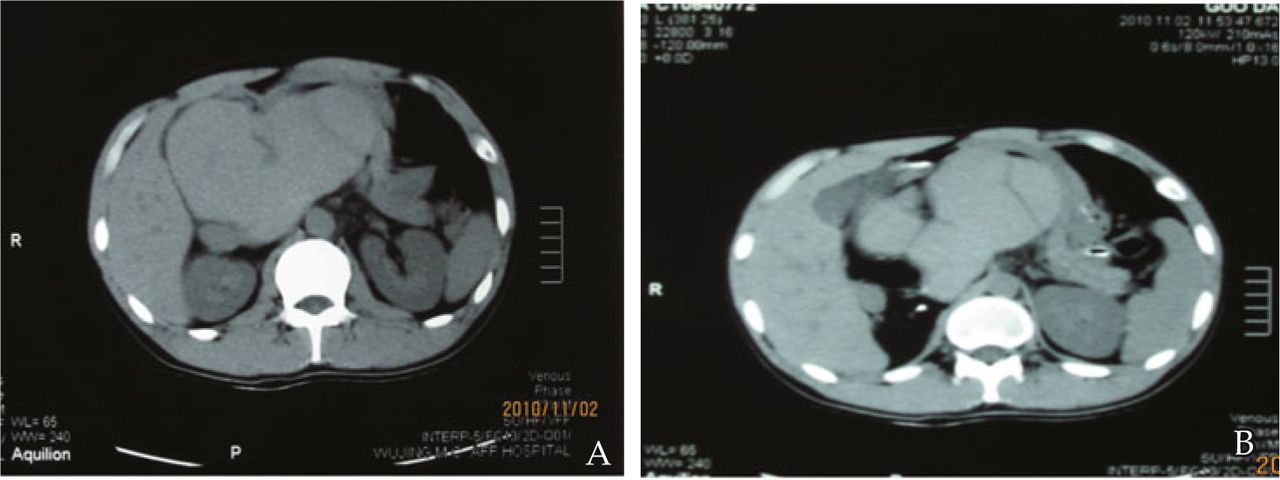
The CT images of a 24-year-old man with 2 masses in the abdominal cavity before operation. A, A huge cystic mass behind the transverse colon, pancrease and stomach, which pushes aside the inferior vena cava and the right kidney; B, This image is characterized by the conflict of 2 different masses in the retroperitoneal cavity.

The specimens taken from the surgery. A, The exsected lesion in the right retroperitoneal cavity. B, The exsected huge cystic mass in the left retroperitoneal cavity.
Discussion
This case indicated that 2 different masses can exit concurrently in the abdominal cavity. The gastrointestinal duplication is a congenital malformation, which can occur throughout the alimentary tract from the mouth to anus, and it often occurs in the jejunal and ileal of pediatric patients, while lesions occurring in the colon are less[8,9]. A mature teratoma is a germ-cell origin tumor (GCTs), which may be consist of mature or immature tissues deriving from 3 pluripotential germ cell layers: ectoderm, mesoderm and endoderm, and it contains cartilage, bone, pancreatic tissue, lymphoid tissue, and skeletal muscle, etc.[10,11] Germ-cell tumors (GCTs) are the most common solid tumors in young men. A non-GCT teratoma has the tendency to malignant transformation. Most teratomas have no symptoms since his birth, and when the bleeding or rupture of teratoma occurs, the abdominal signs can be identified. Teratoma occurs mostly in the gonadal, extragonadal, ovary and sacral regions, and it is rare to occur in the areas near the biliary duct, porta hepatis, or liver [12-14].
The current case was characterized by the conflict of mature teratoma and colon duplication in the retroperitoneal cavity, and the teratoma was located near the common biliary duct. Based on the ultrasound and CT images, the nature of the teratoma was identified before the operation, but the cystic colon duplication wasn’t detected. We only identified that the cystic mass was associated with the alimentary tract, and its image showed unclear and high dense of the cystic wall. Though colonic duplication and teratoma were found in the emergency operation because the diagnosis of peritonitis were confirmed by presenting the symptoms of the abdominal tenderness, abdominal rigidity and rebound tenderness, we should have the mind before the surgery that the coexisting masses in the abdominal cavity could be teratoma and colon duplication.
Conflict of interest statement
No potential conflicts of interest were disclosed.
- Received December 1, 2010.
- Accepted March 1, 2011.
- Copyright © 2011 by Tianjin Medical University Cancer Institute & Hospital and Springer
In this issue






{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.