

keywords
Introduction
Neuroendocrine tumor covers a wide range of neoplasms that originate in the neuroendocrine cells which spread throughout the body. Carcinoid tumor, and neuroendocrine tumor are low-grade malignant tumors, their growth is slow, and mainly in the gastrointestinal epithelium. Esophageal adenocarcinoma tumor is a big problem in esophageal cancer. Combined esophageal adenocarcinoma and carcinoid tumor both as primary tumors is very rare[1].
Neuroendocrine tumors of the esophagus are derived from the diffuse neuroendocrine system in the gastrointestinal tract. Neuroendocrine tumors in the esophagus can be distinguished from other mesenchymal tumors by immunostaining for synaptophysin and chromogranin-A. Both carcinoid of the esophagus and adenocarcinoma of the esophagus are malignant tumors and considered to have a specific molecular pathogenesis. This paper presents a rare case diagnosed as carcinoid of the esophagus concomitant with an adenocarcinoma of the esophagus, a review of the literature is also presented here.
Case Report
In October 2008, a 40-year-old man came to the Affiliated Hospital of Chengde Medical College for a physical examination. He indicated pain in his esophagus when swallowing food. OLYMPUS GIF-XQ260 Esophagogastroduodenoscopy was given and showed an ulcerative-type tumor about 1.5 cm in diameter on the posterior wall of his upper esophagus. Three pieces of biopsy samples were taken through esophagogastroduodenoscopy. Histological examination showed a mucosal tumor in the esophagus. Pathological diagnosis for esophageal malignancy, surgery was performed one week later. During the surgical procedure, an ulcerative-type tumor of grayish white and grayish yellow color, about 1.5 × 1 × 0.8 cm3 in size, with a tough texture was found. The specimen was inserted in 10% formaldehyde and embedded in paraffin after being removed in the surgery. After being cut into 5 μm sections the small pieces of the specimen were deparaffinized and rehydrated for hematoxylin and eosin staining. Cytokeratin, synaptophysin, and chromogranin-A (Beijing Zhongshan Biotechnology Co, LTD, The haidian district of Beijing zhongguancun 6 China) were detected in tumor tissue using 2-step immunohistochemical technique and the Dako Envision system. The positive staining of tumor cells was presented as red-brown granules, which were mainly located in cytoplasm when observed under microscope. Control sections were incubated with normal rabbit serum instead of primary antibody. Hematoxylin and eosin staining showed two types of tumor cells: carcinoid accounting for approx, 50% and adenocarcinoma accounting for the remaining 50%. Carcinoid of the esophagus presented uniform ovoid cells with cordal and small nodal patterns within the esophageal stroma (Fig. 1). The cancer tissue was shaped like rosettes when viewed under the microscope (Fig. 2). The adenocarcinoma tumor demonstrated signet ring cells and small heterogeneous glands within the esophageal stroma (Fig. 3). The immunohistochemical staining showed part of tumor synaptophysin and chromogranin-A positive in tumor cells it was diagnosed as carcinoid of the esophagus (Figs. 4 and 5). Another part of tumor negative for synaptophysin and chromogranin-A tumor cells were positive for cytokeratin (Fig. 6). At the same time adenocarcinoma of the esophagus was diagnosed, a carcinoid of the esophagus concomitant with an adenocarcinoma of the esophagus was pathologically diagnosed. Usually, carcinoma invades deep muscular layers, therefore, no metastatic lymph node was found.

Esophagogastroduodenoscopy showed an ulcerative type tumor about 1.5cm in diameter on the posterior wall of the upper oesophagus.

Carcinoid of the esophagus (about 50%) and adenocarcinoma of the oesophagus, A picture of the two components for this tumor, left for adenocarcinoma, right for carcinoid tumor (H&E stain, × 40).

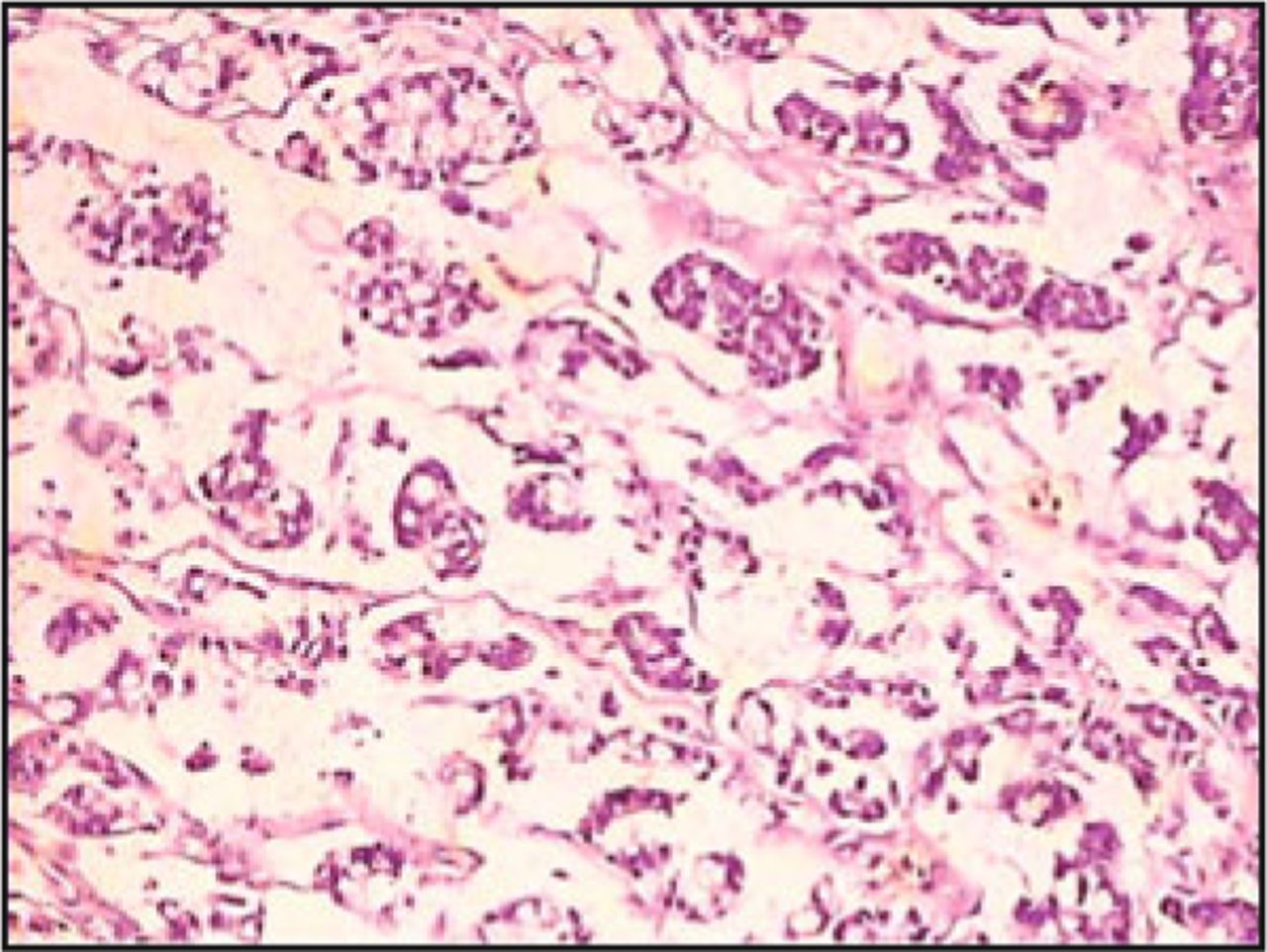
The right for carcinoid tumor presented, carcinoid of the esophagus presented uniform ovoid cells with cordal and small nodal patterns within the esophagus stroma. Cancer tissue was looked like rosettes under microscope (H&E stain, ×100).

The left for adenocarcinoma tumor presented signet ring cells and small heterogeneous gland within the esophagus stroma (H&E stain, ×200).

The right for carcinoid tumor cells showed synaptophysin positive (IHC stain, × 200).

The right for carcinoid tumor showed chromogranin-A positive in tumor cells (IHC stain, ×200).

The left for adenocarcinoma showed cytokeratin positive in tumor cells (IHC stain, × 200).
Discussion
Carcinoid of the esophagus concomitant with adenocarcinoma of the esophagus is clinically rare. To the best of current knowledge, it has not been reported in the literature. The pathogenesis of carcinoid of the esophagus concomitant with adenocarcinoma of the esophagus is unclear.
Carcinoids of the esophagus in different locations on digestive tract may have different clinical features, including esophageal pain, vomiting, and having a choking feeling[2-5]. Carcinoid tumor associated with vascular malformation may cause esophageal bleeding[6,7]. Carcinoids in the digestive tract are classified into 3 subtypes, all of which originate from digestive tract enterochromaffin-like (ECL) cells in the digestive tract mucosa. It is well known that digestive tract ECL cells in the digestive tract mucosa synthesize and secrete 5-hydroxytryptamine (5-HT)[8-11], because the ECL cells tend to become hyperplastic. This causes 5-HT level in the blood to significantly increase, and the carcinoid symptoms are caused by excessive 5-HT level in blood production. Carcinoid syndrome usually includes flushing, diarrhea, but most digestive tract carcinoids are non-functioning neoplasms, and only about 2.4% of patients with digestive tract carcinoids present with carcinoid syndrome. This patient had never experienced any digestive tract symptoms nor carcinoid syndrome. The diagnosis of carcinoid of the esophagus concomitant with adenocarcinoma of the esophagus depended on the features of endoscopic examination, B-ultrasound, computed tomography, endoscopic retrograde cholangiopancreatography (ERCP), endoscopic ultrasonography and pathologic examination, especially immunohistochemical examination for markers, such as synaptophysin, cytokeratin, neuron-specific enolase (NSE), chromogranin-A, epithelial membrane antigen and/or neurosecretory granules, which are observed through electronic microscope.
Carcinoids of the esophagus are preferentially diagnosed as tumors based on the findings of cytokeratin, synaptophysin, chromogranin-A, and positive neurosecretory granules in immunohistochemical staining, which are observed through electronic microscope.
The treatment modality for carcinoid of the esophagus concomitant with adenocarcinoma of the esophagus is surgery[12-18] followed by chemotherapy including chemoembolization, radiotherapy and/or biotherapy. The initial treatment of functioning carcinoid of the esophagus concomitant with adenocarcinoma of the esophagus is to control the symptoms caused by excessive 5-hydroxytryptamine production.
In conclusion, the purpose of this report was to demonstrate this rare case so that other fellows in the field of oncology could learn something from it.
Conflict of interest statement
No potential conflicts of interest were disclosed.
- Received July 11, 2010.
- Accepted August 18, 2010.
- Copyright © 2010 by Tianjin Medical University Cancer Institute & Hospital and Springer
In this issue






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.