

Abstract
OBJECTIVE To evaluate the efficacy and adverse effects of gemcitabine versus pegylated liposomal doxorubicin in patients with progressive or recurrent ovarian cancer.
METHODS We conducted a systematic literature search to identify all randomized controlled trials comparing gemcitabine and pegylated liposomal doxorubicin for progressive or recurrent ovarian cancer. Trial data were reviewed and extracted independently by 2 reviewers. We evaluated the quality of the included studies using the Handbook 5.0 recommend standards and then analyzed data by Cochrane Collaboration’s RevMan 5.0.
RESULTS Two trials which included a total of 348 patients were analyzed. The results of meta-analysis showed that gemcitabine improved disease control rates significantly bett er than pegylated liposomal doxorubicin. A greater number of patients receiving gemcitabine experienced neutropenia compared with patients receiving pegylated liposomal doxorubicin; however, hand-foot syndrome and mucositis were more severe in patients receiving pegylated liposomal doxorubicin.
CONCLUSION Gemcitabine provided a limited advantage compared with pegylated liposomal doxorubicin. There exists an urgent need for more high-quality, multicenter, adequate randomized, controlled clinical trials for comparing gemcitabine with pegylated liposomal doxorubicin in patients with progressive/recurrent ovarian cancer.
keywords
Introduction
Ovarian cancer is the second most common of gynecological malignancies and represents the leading cause of death among all gynecological tumors. Approximately 21,550 new cases are expected to be diagnosed and nearly 14,600 women are expected to die from the disease in the United States in 2009[1].
Currently, the standard primary therapy for advanced ovarian cancer involves a combination of maximal cytoreductive surgery and chemotherapy with carboplatin plus paclitaxel or with carboplatin alone. However, of all patients with the disease, more than 60% develop a relapsed or resistant disease[2-5]. Patients are usually incurable regardless of progression or recurrence; therefore, the goal of therapy is improvement in both length and quality of life, resulting in a therapeutic challenge. Consequently, the urgent finding active agents for patients with progressive or recurrent disease following platinum-based chemotherapy has been urgently pursued. Options for second-line therapy include gemcitabine (Gem), topotecan (Top) and pegylated liposomal doxorubicin (PLD)[6], and in consideration of the limitations inherent in the comparison of response rates across phase III studies, none of the drugs has show superiority over the others[7-11].
Gemcitabine has undergone investigation as a second-line chemotherapy in a series of clinical trials that have demonstrated its safety and efficacy. Different schedules of treatment have been used with a drug dosage ranging from 800 to 1,250 mg/m2 weekly for 3 weeks followed by a 1-week rest, depending on prior chemotherapy and toxicity. Some studies of gemcitabine monotherapy for platinum-resistant/recurrent ovarian cancer have proven activity, with overall response rates between 14% and 22%; the median duration of response has ranged from 4.0 to 10.6 months[10-15]. PLD is another active agent indicated for the treatment of ovarian cancer that is refractory to paclitaxel/platinum-based regimens which is given intravenously at a dose of 40-50 mg/m2, once every 4 weeks. Response rates to these second-line agents has ranged between 12% to 14% for women with platinum refractory ovarian cancer[10,11]. The main toxicities are palmar-plantar erythema (redness and soreness of the palms, hands and soles of feet), sore mouth, low blood counts and cardiotoxicity.
Since both of the 2 agents have shown promising activity with different adverse effects, which of them is superior in the treatment of progressive or recurrent ovarian cancer over the other agent? A systematic review of the literature was conducted to compare the efficacy and safety of gemcitabine versus PLD in women with progressive or recurrent ovarian cancer.
Materials and Methods
Literature search
We searched PubMed (1966-2009), EMBASE (1974-2009), the Cochrane library (2009 issue 3), Chinese Biomedical Literature Database (1978-2009), the online proceedings of the American Society of Clinical Oncology (ASCO) Annual Meetings (1992-2009) and Google Scholar et al. The search strategy was “(ovarian neoplasm or ovarian cancer or ovarian tumor or ovarian carcinoma) AND (gemcitabine or GEM or gemzar) AND (pegylated liposomal doxorubicin OR doxorubicin OR doxil)”. Two reviewers conducted the search independently, and they also evaluated study quality using Cochrane recommendations. Disagreement was resolved by discussion with others.
Inclusion criteria
Types of studies
We included all randomized trials of gemcitabine vs. liposomal doxorubicin for progressive/recurrent ovarian cancer as second-line treatment.
Types of participants
Patients ≥ 18 years of age of any ethnic origin with measurable or assessable progressive/recurrent ovarian cancer.
Types of outcome measures
The main endpoints were effect outcome reported in terms of progression free survival (PFS), time to progression (TTP), and overall survival rate (OS). Other measures included objective response rate (ORR), disease control rate (DCR) and adverse effects (AEs).
Data extraction
The review was undertaken by 2 reviewers. The search strategy described above was developed and performed to identify eligible studies. The results were combined and all titles, abstracts, or when necessary the full text, were screened independently by 2 authors. In cases of disagreement between the 2 authors, the full article was obtained and inspected independently by a third author. Data extraction was carried out by the same reviewers independently using standard data extraction forms. Studies reported in non-English language journals were translated before assessment. When more than one publication of one trial existed, only the publication with the most complete data was included. Any further information required from the original author was requested by written correspondence and any relevant information obtained in this manner was included in the review. Any discrepancies were resolved by discussion.
Quality evaluation
The quality of studies was assessed independently without blinding to authorship or journal using the checklist. Discrepancies were resolved by discussion.
The quality items assessed were sequence generation, allocation concealment, blinding of participants, personnel and outcome assessors, incomplete outcome data, selective outcome reporting and other sources of bias. We recorded problems in respect of these issues in full, and for individual studies each criteria was assigned a label of ‘yes’, ‘unclear’ or ‘no’ to estimate risk of bias.
Statistical analysis
Quantitative meta-analyses were performed to assess the differences of efficacy and adverse effects between 2groups. Statistical analysis was performed and the forest plots were generated using the Review Manager (version 5.0) software application. The risk ratio (RR) was calculated along with its 95% confidence intervals (CI) for dichotomous outcomes and weighted mean difference (WMD) or standard mean difference (SMD) was calculated for continuous outcomes. Statistical heterogeneity between studies was assessed by means of chi square and the extent of inconsistency was assessed by the I2 statistic. When I2 < 40%, heterogeneity was considered as questionably important; 30%-60% was thought to possibly represent moderate heterogeneity; 50%-90% was regarded as possible substantial heterogeneity; and higher than 75% was deemed a considerable level. A fixed-effect model was used for calculations of summary estimates unless significant heterogeneity existed, in which case a random-effects model was applied. Descriptive techniques were used when clinical heterogeneity existed and also when no data could be used in statistical analysis.
Results
Study selection
We reviewed 55 studies. Fifty-three studies were excluded for the following reasons: 34 had irrelevant content; 10 were single-arm clinical trials; 3 appeared repeatedly; 6 were reviews. Two studies which were randomized controlled clinical trials with a total of 348 patients, were included.
Included trials
Both trials were phase III randomized clinical trials[10,11].
The characteristics and quality of the included studies are shown in Table 1 and Table 2.
Characteristics of included studies.
Assessment quality of included studies.
Outcomes
Objective response rate (ORR: CR+PR)
There existed heterogeneity between the included trials (χ2 = 2.18, P = 0.14, I2 = 54%), so a random-effects model was applied. The results of meta-analysis showed no significant difference between the GEM and PLD groups with regard to ORR [RR = 1.25, 95% CI (0.52, 3.30)] (Fig. 1).

Overall response rate.
Disease control rate (DCR: CR + PR + SD)
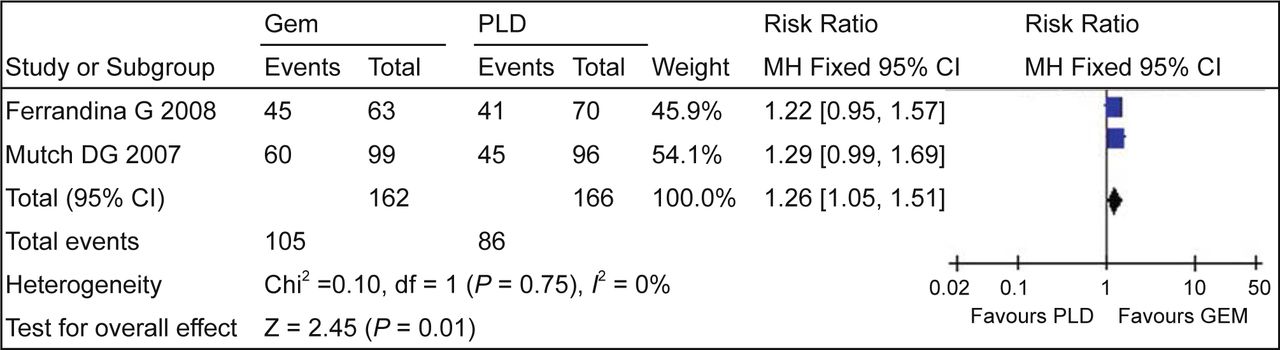
There was no heterogeneity between the included trials (χ2 = 0.10, P = 0.75, I2 = 0%), so a fixed-effect model was used for calculation. The results of meta-analysis showed that the DCR was higher with patients receiving GEM than with patients receiving PLD [RR = 1.26, 95%CI (1.05,1.51)] (Fig. 2).

Disease control rate.
Grade 3/4 myelosuppression
There were no heterogeneities between the included trials with regard to grade 3/4 myelosuppression, so a fixed-effect model was used for calculation. The results of meta-analysis showed that a greater number of patients receiving GEM experienced grade 3/4 neutropenia [RR = 3.00, 95% CI (1.72-5.23)] compared with patients receiving PLD, and no significant difference between GEM and PLD groups with regard to 3/4 thrombocytopenia [RR=1.93, 95% CI (0.67, 5.53)] and 3/4 anemia [RR = 1.35, 95% CI (0.46, 4.00)] (Fig. 3).
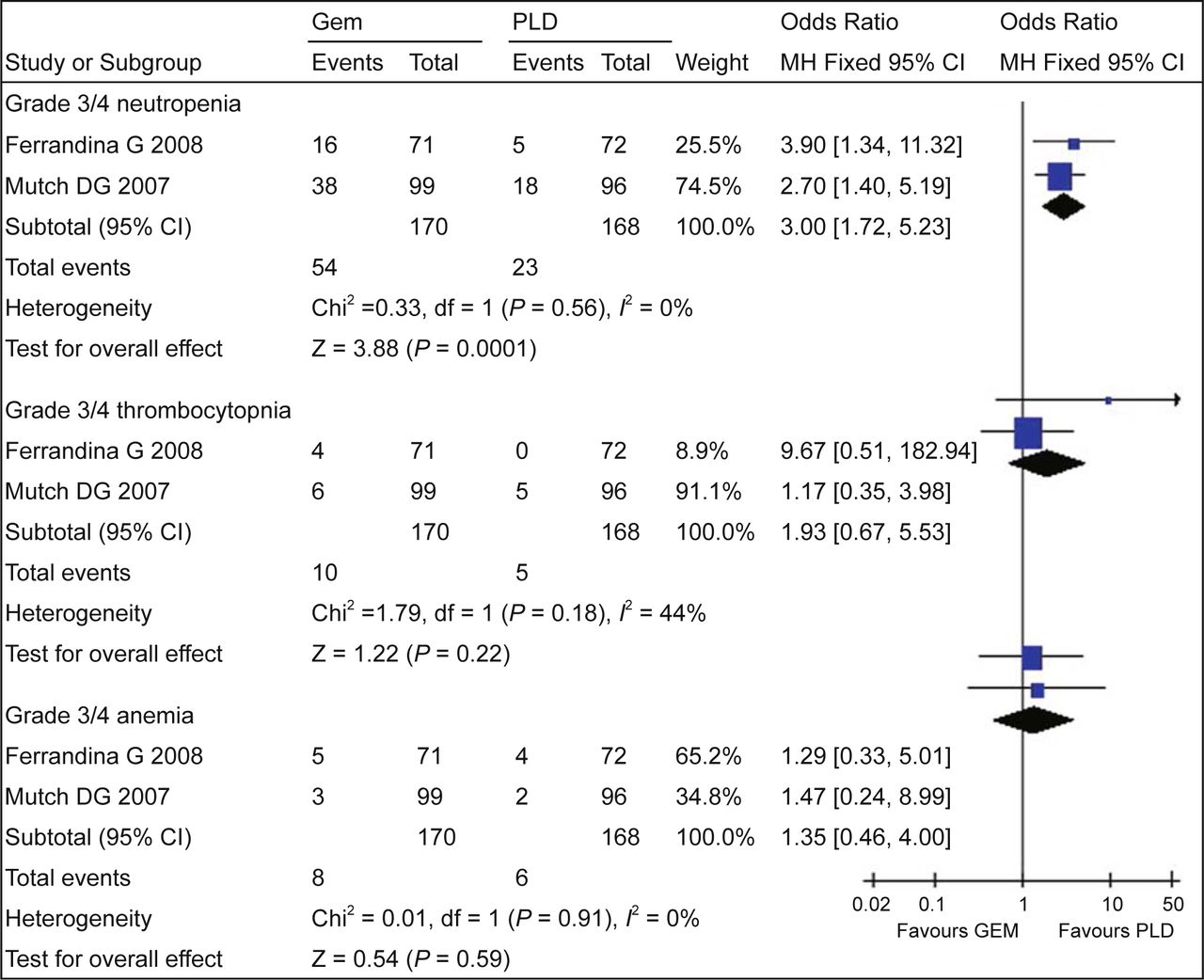
Grade 3/4 myelosuppression.
Other adverse effects
There existed substantial heterogeneity between the trials included (χ2 = 2.24, df = 1, I2 = 75%), so a random-effects model was applied. The results of meta-analysis showed no significant difference between the GEM and PLD groups with regard to grade 3/4 nausea and vomiting [RR = 1.03, 95% CI (0.10, 11.12)]. There was no heterogeneity between the included trials (χ2 = 0.07, P = 0.79, I2 = 0%), so a fixed-effect model was used for calculation. The result of meta analysis showed no significant difference between GEM and PLD groups with regard to grade 3/4 mucositis [RR = 0.40, 95% CI (0.08, 2.01)]
There was no heterogeneity between the included trials (χ2= 0.19, P = 0.66, I2 = 0%), so a fixed-effect model was used for calculation. The results of meta-analysis showed the grade 3/4 hand-foot syndrome was more severe with patients receiving PLD than patients receiving GEM [RR= 0.07, 95% CI (0.01, 0.49)].
PFS, TTP, OS, QOL
Mutch et al.[11] reported that the median PFS was 3.6 vs. 3.1 months and that the median OS was 12.7 vs.13.5 months in the G and PLD groups, respectively. Neither showed a statistically significant difference. However, OS data should be interpreted with caution as a result of the cross-over treatment design. Ferrandina et al.[10] reported that there was no statistically significant difference in TTP curves between 2 groups (20 vs. 16 weeks, P = 0.411). A trend towards a more favorable OS was documented in the PLD group compared with the G group, although the trend was of borderline statistical significance (56 vs.51weeks, P = 0.048).
Discussion
Two prospective randomized controlled phase III trials comparing gemcitabine with pegylated liposomal doxorubicin in patients with progressive or recurrent ovarian cancer have been reported in the literature. The quality of both included trials was relatively low, which might contribute high bias. One trial[11] mentioned the method of randomization but did not describe it in detail. The trial did not utilize blinding, while in the other trial[10], only evaluators were blinded, which might produce performance bias and measuring bias. Neither trial included reported adequate concealment of allocation of outcomes assessment, which might bring selective bias.
There were significant differences in the disease characteristics between the 2 studies. Patients in the study by Mutch et al.[11] appeared to have platinum-resistant ovarian cancer. In addition to patients experiencing treatment failure with one first-line platinum/paclitaxel containing chemotherapy, the trial by Ferrandina[10] trial also included the patients who experienced recurrence or who were once platinum-sensitive. The study by Mutch et al.[11] was not designed as an equivalency study, as the median CA-125 value for assessable patients at baseline was higher for the gemcitabine group (525.2 U/ml) compared with the PLD group (291.3 U/ml). It seemed to be an unfavorable situation for the Gem group. That might be a reason for the significant heterogeneity between 2 trials in ORR. In such a disadvantageous situation, gemcitabine improved DCR over PLD significantly. We could consider that gemcitabine was more effective than PLD. Neither PFS nor TTP in each trial showed a statistically significant difference. In the study by Ferrandina et al.[10], a trend towards a more favorable OS was documented in the PLD group rather than in the G group with borderline statistical significance. Therefore, there exists an urgent need for additional high-quality, multicenter, adequately randomized, controlled clinical trials for Gem compared with PLD in the treatment of progressive or recurrent ovarian cancer.
In addition, a greater number of patients receiving gemcitabine experienced neutropenia compared with patients receiving PLD; however, the incidence and severity of PPE and mucositis are generally much greater with the use of PLD. Erythema and pain to the palms and/or soles can progress to desquamation reminiscent of burns. The extreme form of this syndrome includes diffuse skin involvement, a syndrome referred to as diffuse toxic erythema[10]. This suggests that Gem was similar in activity to PLD in the patients with manageable toxicities.
Conclusion
Gemcitabine provided a limited advantage compared with pegylated liposomal doxorubicin for patients with progressive or recurrent ovarian cancer. However, the number of included studies was too small such that the universality of the results might be affected.
- Received December 7, 2009.
- Accepted November 23, 2009.
- Copyright © 2009 by Tianjin Medical University Cancer Institute & Hospital and Springer
References
In this issue






{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.