

Abstract
OBJECTIVE To assess the use of gluteus maximus muscle to reconstruct the anal sphincter for very low rectal cancer. This study aimed to evaluate the local recurrence and function of the new anal sphincter after operation.
METHODS Sixteen patients underwent the replacement operation, and then received biofeedback treatments 1 month after the operation. The therapeutic responses were evaluated using the Vaizey and Wexner scoring systems and vectorial manometry. The controls were 30 cases who had undergone a low anterior resection for rectal cancer and 30 healthy people.
RESULTS Median follow-up was 4.2 years. No local recurrence was observed. The Vaizey and Wexner scores and vectorial manometry 1 month after operation were significantly lower than those of the healthy and low anterior resection controls ( P <0.001). After biofeedback treatments, the above indexes improved significantly ( P <0.001), especially after 1 year ( P <0.001), but still remained lower than the controls( P <0.001). The rectoanal reflex only increased to 31.3 % 1 year after operation.
CONCLUSION The local recurrence after the replacement operation was low. The defecation function was poor early after operation, but increased markedly after biofeedback treatments and long-term functional exercise. This therapy can be one choice for very low rectal cancer.
keywords
Radical surgical removal of the tumor is the main objective for a permanent cure of rectal cancer. Apart from this, the preservation of fecal continence is the second most important goal to reach an acceptable quality of life. Although approximately one-half of the tumors are localized in the upper third of the rectum, patients with a cancer localized in the middle or lower third are still confronted with the possibility of a permanent colostomy. There are two kinds of anoplasty for rectal cancer located at or near the anorectal junction. One is a direct coloanal anastomosis without any replacement, while the other is a different replacement for the sphincter. Intersphincteric resection(ISR)[1~4] is employed in the former technique, while for the latter, there are artificial replacements(eg. memory alloy) and autogeneic sphincter replacements(eg. gracilis muscle) [5]. Every technique has its positive features and limitations, and up to now, there is still no accepted perfect operation.
This report describes the technique of using gluteus maximus muscle to replace a sphincter to reconstruct the anus for very low rectal cancer, and using biofeedback treatment to train the anal function after operation. The objective of the study was to use a subjective scoring system and vectorial manometry to evaluate the function of the new anal sphincter, and to assess possible local recurrence with a long-term follow-up.
METHODS
Patients
From September 1997 to July 2005, 16 patients underwent the gluteus maximus replacing sphincter operation. There were 4 males and 12 females, with a median age of 58.7 (42-65) years. All 16 patients had tumors located between 1.0~4.0 cm from the anal verge (average 2.3 cm). The distance was measured with a rigid sigmoidoscope with the patient placed in a lateral position. The transversal size of tumors was less than 1/2 the circumference of the rectum. The TNM staging was evaluated by digital examination, colonoscopy with biopsy, endorectal ultrasonography (uTNM), and MRI (which used after January 2004). The findings showed patients had 13 T3 tumors and 3 T4 tumors for pathologic grading, 10 G1 tumors and 6 G2 tumors for histological grading. Median follow-up was 4.2(0.4~7.1) years. There were 30 controls selected who had undergone a low anterior resection for rectal cancer (LAR controls) and 30 controls who were healthy people (normal controls).
Surgical technique
The operation was performed in a lithotomy position. After complete dissection of the rectum and mesorectum down to the pelvic floor, the anal part of the operation was started. Suturing and distracting the circumferential skin guarantees easy access to the region, then the anal orifice is closed from the inferior margin of the tumor to the superior margin of the opposite side dentate line. An incision in the anoderm at the opposite side of the tumor facilitates the exposure of the internal sphincter. The next step is an incision in the internal sphincter and separation from the homolateral external sphincter and puborectalis. Preserving at least 1/3 of the circumferential sphincter, the tumor part is dissected just as in a Miles’ operation. After macroscopic inspection, the specimen is sent to pathology. If the incisal edge has residual malignant cells, a Miles’ operation is continued.
For a negative incisal edge, the following procedure is conducted. A radiate incision is made on the tumor side, and a bundle of gluteus maximus muscle is dissociated preserving the neurovascular bundle near the anal canal, which is used to replace the resected sphincter, then the neosphincter is formed. The sigmoid or descending colon is pulled down through the new anal canal and the coloanal anastomosis is situated by 3-0 absorption line below the dentate line. The caliber of the new anal canal should just permit passage of the forefinger. Finally, a catheter encysted by petrolatum gauze to permit deflation is secured before anastomotic stoma healing.
Biofeedback training scheme
One month after operation, the proper training was selected to improve defecation function. Biofeedback training was used to strengthen the anal muscles, and to improve the sensations in the rectum and coordination of the external anal sphincter. For this purpose electrostimulation was combined with biofeedback training.
Vectorial manometry
The instrumentation used was the PC Polygram HR and pressure transducer produced by the Sweden CTD-SYNECTICS Co. The analytical system employed was comprised of the vectorial manometry software offered with the instrumentation, and the infusing system used a low compliance water perfusion, and a nitrogen pressure maintenance 40 kPa. Pure distilled water served as the conduction medium, with the drop number held at 0.5 ml/min. The manometric catheter offered was an eight-channel polythene catheter. The manometry was executed by a stationary pull-thorough technique at 0.17 cm/s. The indexes recorded include maximum pressure, vectorial manometry, sphincter asymmetry index (SAI), and rectoanal reflex.
Incontinence assessment
Patients were assessed with the use of validated Vaizey and Wexner scoring cards. The Vaizey scale is a 24-point measure of fecal incontinence. Patients with a score of zero are considered to have normal continence[6]. The Wexner scale is a 20-point assessment of fecal continence and likewise a score of zero is considered to be normal[7].
Statistical analysis
Data are presented as the mean(±standard error). Comparisons of parametric data were performed by the t-test, and statistical analysis was performed using the SPSS for Windows statistical software package.
RESULTS
Follow-up
Follow-up examinations were performed every 3 months for 2 years postoperatively, and after that every 6 months. Median follow-up was 4.2 (range, 0.4 ~7.1) years, with only one patient being lost to follow-up after 6 years. Most of the patients (75%) were observed for at least 24 months. All patients received chemotherapy with the FOLFOX4 scheme with no patients developing a local recurrence. However one patient had a solitary liver metastasis at 13 months postoperatively, which was treated with a curative partial hepatic resection, but then was lost to follow-up after 6 years postoperatively.
Vaizey and Wexner Scores
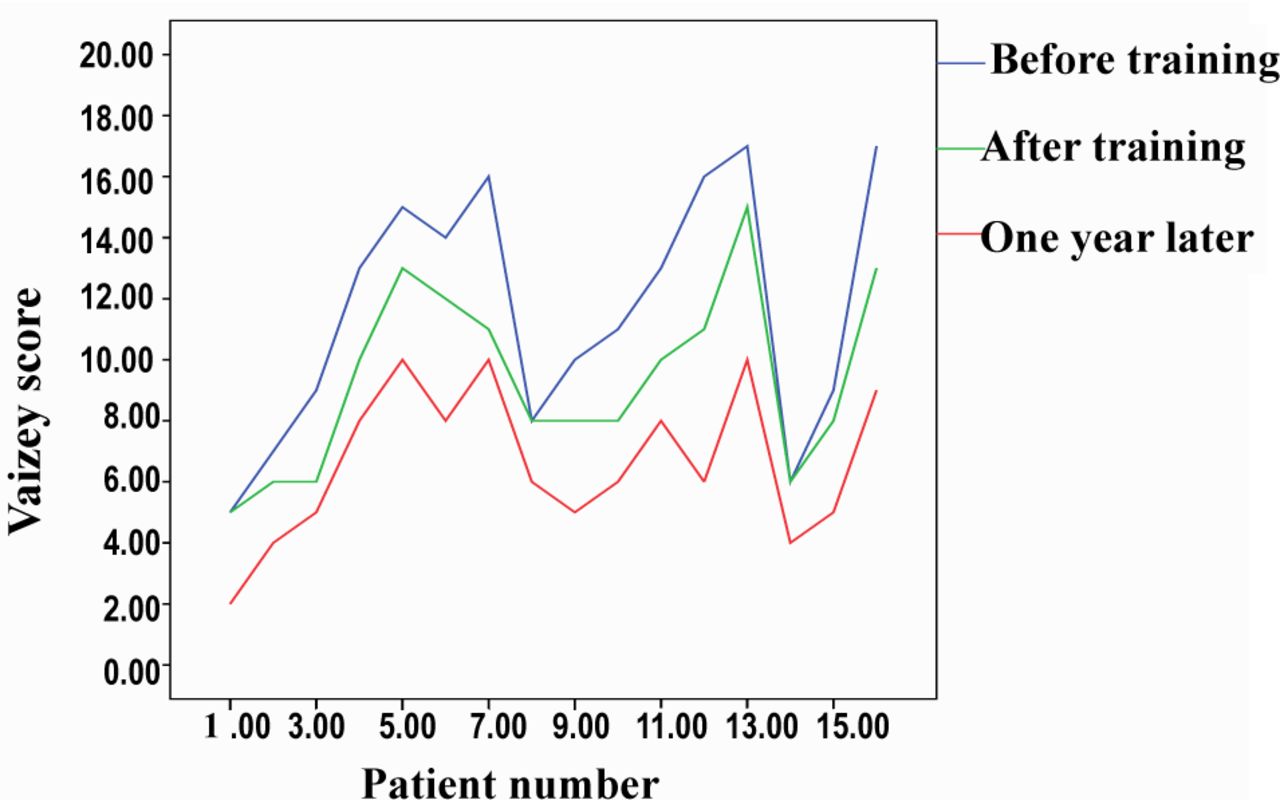
All patients received postoperative biofeedback training after 4 weeks. The Vaizey and Wexner scores were assessed in 16 patients. The mean Vaizey score before biofeedback therapy was 11.6 (range 5~17) and after biofeedback was 9.4 (5~13), then reaching 6.6(2~10) after 1 year. This represented a significant improvement in patient continence (P<0.001) (Fig.1). The mean Wexner score before biofeedback therapy was 10.1 (range 5~15). After biofeedback training it was 8.4 (4~12), and after 1 year achieved 5.7(2~9). This again represented a significant improvement in patient continence (P<0.001) (Fig.2). In total, 81.3% of the patients had a significant improvement in their Vaizey and Wexner scores after biofeedback training. Especially 3 years later, the mean Vaizey score was 4.9 and Wexner score was 4.0 for 9 patients who were followed-up. And for 4 patients who were followed-up for 5 years, the mean Vaizey score was 3.7and Wexner score was 2.8. Most patients were satisfied about their defecation function.

The Vaizey score before and after biofeedback training and one year later.

The Wexner score before and after biofeedback training and one year later.
Vectorial manometry
All patients underwent anorectal vectorial manometry before and after biofeedback therapy, and again 1 year later (see Table 1). All indexes 1 month after operations were significantly different compared to the normal and LAR controls. The maximum squeezing anal pressure and squeezing vector volume represented a significant improvement after biofeedback training (p<0.001), but the maximum resting anal pressure (p=0.334) and resting vector volume (p=0.623)did not show a significant difference. The indexes improved significantly one year later(p<0.001), but did not reach the normal level (p<0.001), even when compared to the LAR control(p<0.001). The percentage of SAI decreased from 78.3% to 71.9% in the relaxation period (p<0.001) and from 58.3% to 45.5% in the contraction period (p<0.001) after biofeedback training. One year later, the SAI decreased significantly but was still higher than the normal control. No patients could detect a rectoanal reflex after operation, and after the biofeedback therapy, only two patients had a weakly positive reflex, and up to 1 year later, 5 patients developed the normal rectoanal reflex (31.3%).
The vectorial manometry results before and after biofeedback training and one year later.
The SAI* results before and after biofeedback training and one year later.
DISCUSSION
With advances in rectal anastomotic techniques, sphincter preserving operations have become usual for rectal cancers which are located farther away than 5 cm from the anal edge, but permanent colostomy is still performed in about 20% of rectal cancer patients, which results in serious psychologic and social limitations[8,9]. For this reason, different anoplasty has been applied to improve the quality of life for those patients. But still, no technique has satisfactory results, especially related to fecal incontinence.
Biofeedback has been used extensively in clinical practice to treat fecal incontinence, as indicated by a systematic literature search which found 46 studies using biofeedback to treat adult patients complaining of fecal incontinence. The search revealed that 48.6% of the patients were said to be cured of symptoms of fecal incontinence after biofeedback therapy and 71.7% of the patients indicated improvement[10]. But some randomized, controlled studies could not support the effect of biofeedback therapy[11], moreover there is little standardization of biofeedback treatment, and methodologically rigorous evidence for its effectiveness is lacking[12]. Therefore there is a need for objective definitive studies rather than subjective reviews. In our study we preserved a normal sphincter, making the neosphincter synergistically from type I and type II muscle fibers. For this reason, the antifatigue of the neosphicter can improve, and the defecation function also can improve by feedback therapy which stimulates the type II muscle fibers to transform into type I muscle fibers.
Most patients feel dissatisfaction with their defecation function 1 month after operation. The results of incontinence assessment and vectorial manometry can not be favorably compared with the normal controls even with the LAR controls. After the feedback training, 81.3% of the patients showed a significant improvement. The maximum squeezing anal pressure and squeezing vector volume increased significantly after the feedback therapy, which indicated that the feedback therapy can reinforce the antifatigue of the neosphincter. At the same time, the anal manometry showed no apparent change of the maximum resting anal pressure and resting vector volume, which may be because the resting pressure is due 55% to the internal sphincter, 15% to the hemorrhoidal plexus, and 30% to the external anal sphincter[13]. All of the internal sphincter and hemorrhoidal plexus were resected in the operation. Therefore the resting pressure can not have a significant change in the short term. One year post operation, all indexes had a significant improvement, even for resting pressure. The mean Vaizey score was 6.6 and Wexner score was 5.7, so 75% of the patients were satisfied with their defecation function. However 2 patients still complained about their poor discernibility for gas and liquid. Another 2 patients expected their liquid controllability could be improved. The continuous feedback therapy for 4 patients produced no significant improvement, but 1 patient did obtain a relatively satisfactory function at 23 months later, while the other 3 patients maintained the same state until now.
The sphincter asymmetry index is a special index of vectorial manometry, which raised up significantly after the operation. Even in normal people, the anal pressure distribution is longitudinally and transversally asymmetrical[14]. However, the neosphincter which is made up from the 2 muscle fibers has a completely different intensity and antifatigue reaction, so the increase of the SAI can hardly be avoided. After the feedback training, the SAI decreased markedly both in the relaxation period or in the contraction period, but still had a significant difference compared to the normal controls. As for the rectoanal reflex, all the patients had a negative reflex after operation. This is because the entire internal sphincter was resected. However the injury to the internal sphincter may cause a rectoanal inhibitory reflex[15]. There were 12.5% of the patients who showed a weak positive reflex after feedback training, and 31.3% of the patients unexpectedly developed a rectoanal reflex one year later, showing that there are other factors that affect the rectoanal reflex.
On the whole, local recurrence is low after using gluteus maximus muscle to reconstruct the anal sphincter for very low rectal cancer. The defecation function is poor in the short term, but can be markedly improved after feedback training and long-term functional exercise. This operation can be one choice for very low rectal cancer.
Footnotes
This work was supported by a grant from the University Science and Technique Research Program of the Education Department of Liaoning Province(No.05L484)
- Received March 1, 2007.
- Accepted March 26, 2007.
- Copyright © 2007 by Tianjin Medical University Cancer Institute & Hospital and Springer
In this issue






{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.