

Abstract
OBJECTIVE To assess the significance of sentinel lymph node biopsy (SLNB), serial section and cytokeratin immunohistochemical staining in the diagnosis and staging of Stage-cN0 oral squamous cell carcinoma (OSCC).
METHODS A blue stain, 99mTc-dextran SPECT lymphoscintigrapgy and intraoperative γ-ray probes were used to examine the sentinel nodes in 31 cases with Stage-cN0 oral cancer. The H&E staining and a cytokeratin AE1/AE3 immunohistochemistry (IHC) assessment, with serial sections, were conducted to provide results obtained from a routine pathological examination of lymph nodes. The value of the routine pathological examination of the sentinel lymph node (SLN), serial sections and IHC determination for cervical lymph node metastasis of Stage-cN0 OSCC was appraised.
RESULTS A total of 45, 55 and 51 SLNs were examined in 25 (80%), 31 (100%) and 30 (96.5%) of the cases, by using the blue stain, γ-ray probes, and SPECT lymphoscintigraphy, respectively. The average SLNs found in each case of the groups was 1.4 (1 to 3) and there were 1,302 non-NSLNs. Six positive SLN metastases were detected by routine pathological examination, among which 1 case was found to be an accompanied positive metastasis of non-SLN. One positive SLN metastasis was found after examination of serial sections plus routine H&E staining and 2 were detected using serial sections plus AE3 immunohistochemical staining methods. No positive NSLNs were found in the study.
CONCLUSION In order to make more progress in accurate SLNB diagnosis, serial sections and IHC (AE1/AE3) methods can be used for examination of the micrometastases which are difficult to identify by routine pathological sections and H&E staining.
keywords
INTRODUCTION
Whether or not there are metastases of cervical lymph nodes is an important factor for prognosis of oral carcinoma patients, and also is a key reference for developing an operation program. The data from Stage-cN0 patients have indicated that recurrences after operation account to 15% to 60%, and that the level of imperceptible metastasis of Stage-cN0 patients may reach 20%[1]. With an extensive application of SLNB technology, the concept of SLN has been accepted by more and more clinicians. So, ascertainment of the real condition of cervical lymph nodes becomes especially important. In our study, we utilized routine pathological examinations of SLN to appraise the detecting ability of SLNB for cervical lymph-node metastasis of the Stage-cN0 patients with oral carcinoma. At the same time, serial sections of the lymph nodes were made for IHC examinations with the possibility of enhancing the detection rate of metastatic cervical lymph nodes of the OSCC Stage-cN0 patients.
MATERIALS AND METHODS
Patients
Thirty-three OSCC patients received no previous therapy. The sex ratio between the patients was 19 males and 12 females, with a mean age of 56.3 (47 to 76) years. Among the patients, lingual cancer accounted for 12 cases, plus 7 carcinomas of the cheek, 7 of the gingiva, 3 of carcinoma of the mouth floor and 2 of the jaw. Based on the UICC clinical stage, 18 of the total cases were classified as Stage-T1 and 13 as Stage-T2. No intumescent lymph nodes were clinically palpable, and evidence for cervical lymph-node metastases was not found in the cervical type-B ultrasonic inspection, CT or MRI scan.
Drugs and injections
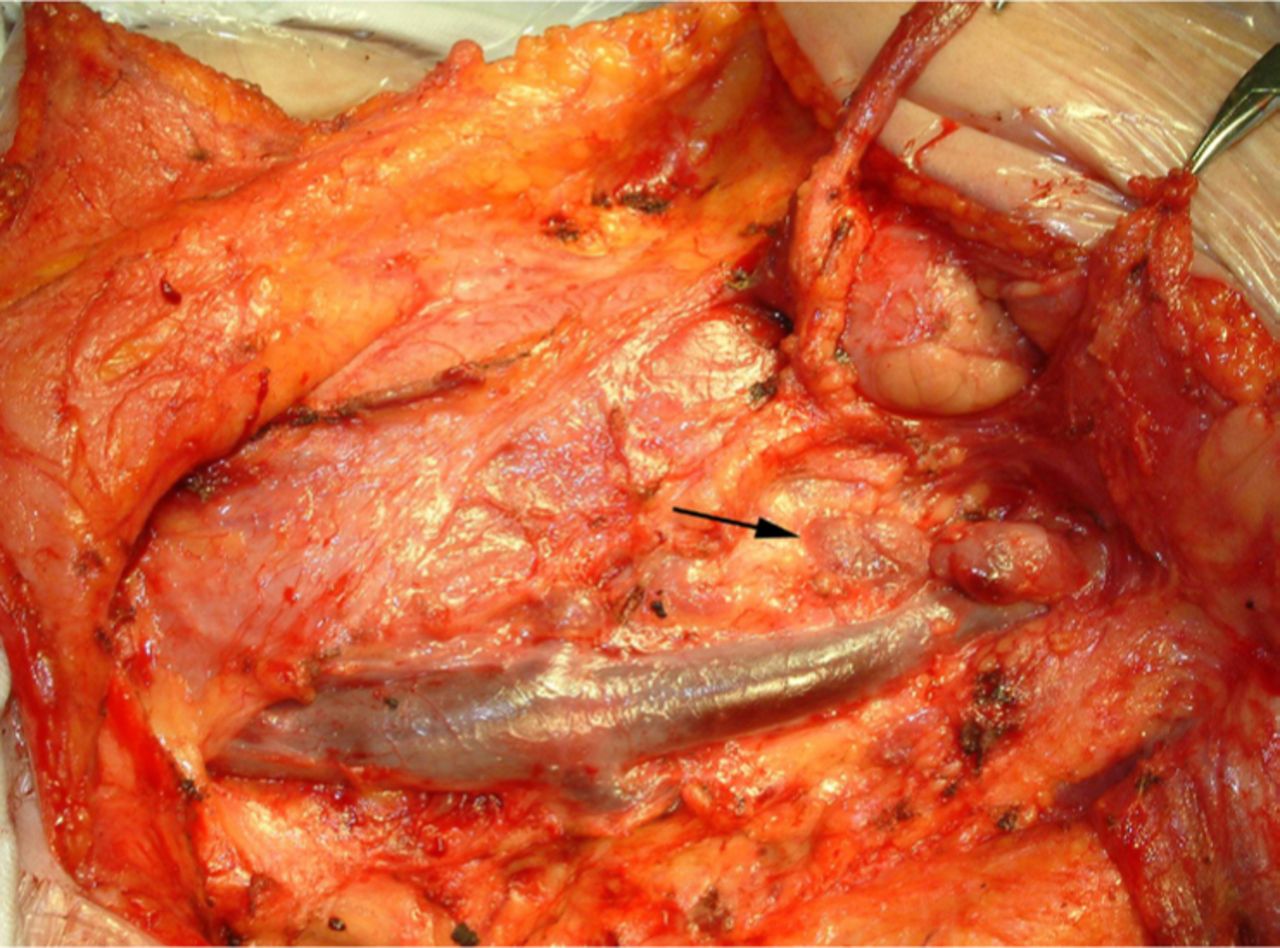
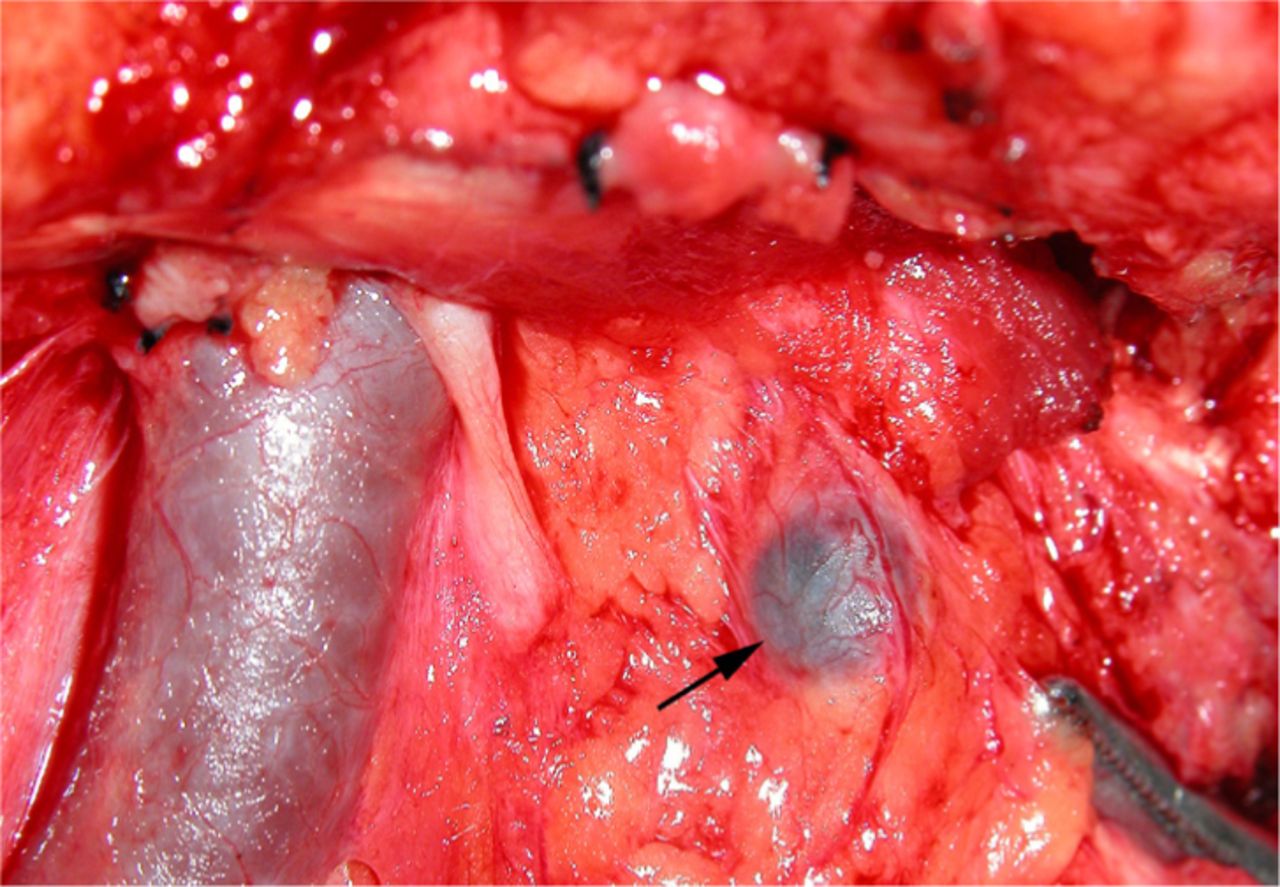
The 99mTc-DX (Dextran), a radioactive drug, was supplied by the Beijing Senke Pharmaceutical Co. Ltd. The relative molecular mass was 100,000 and granule size of 100 to 200 nm, with a labeling rate of more than 95% and a specific radioactivity of 370 MBq/ml. A 0.2 ml of a solution of 99mTc-DX was submucously injected at points 3, 6, 9 and 12, 5 mm away from the tumor, with a withdrawing of the needle to prevent extravasation after the injection. Then the patient was requested to rinse their mouth with clean water. After general anaesthesia and 15 min before the operation, a submucosal 0.2 ml injection of the patent blue violet (Sigma Chemical CO.P.O.) was conducted at points 3, 6, 9 and 12 that were 5 mm away from the tumor, in order to observe the blue staining of the lymph nodes and to record the position and size of the lymph nodes (Figs.1,2).
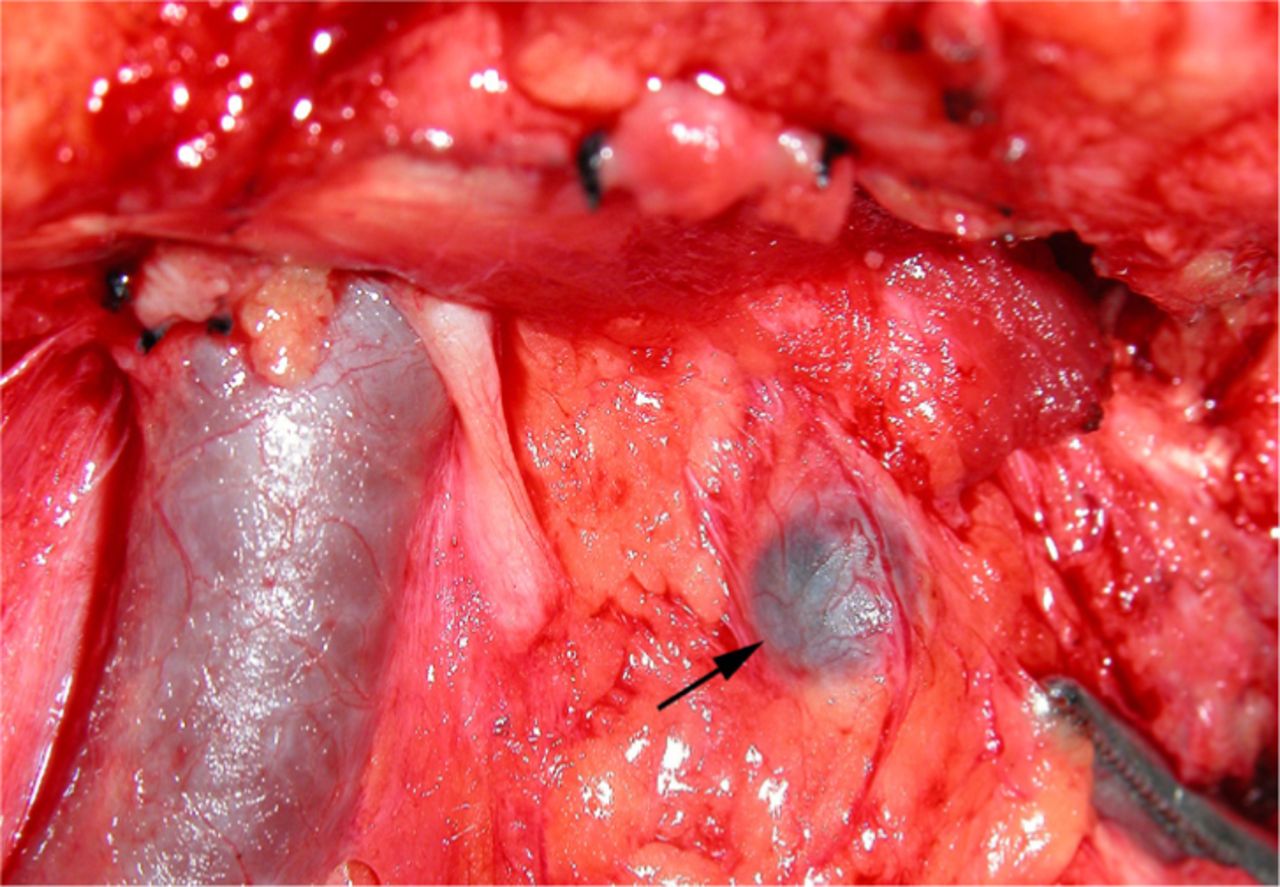
The blue-staining SLN is seen at upper area of the deep part of neck during neck dissection.

Two SLN identified by the blue-stain method.
ECT Lymphoscintigrapgy
Imagescope: Manufactured by the German Simens Co. (ECAM SPECT), with a parallel aperture collimator of low energy expenditure and high resolution. A planar image was shown 15, 20, 30, 45 and 60 min after injection, with a matrix of 256×256 and a frame frequency of 200 KC/frame. After appearance of the lymph node image, the labeling was performed on the mastoid process, angle of the jaw, submentum and suprasternal notch, employing radioactive point sources, so as to find the position of the lymph nodes and mark them respectively at the dermatic surface.
The γ-probe detection
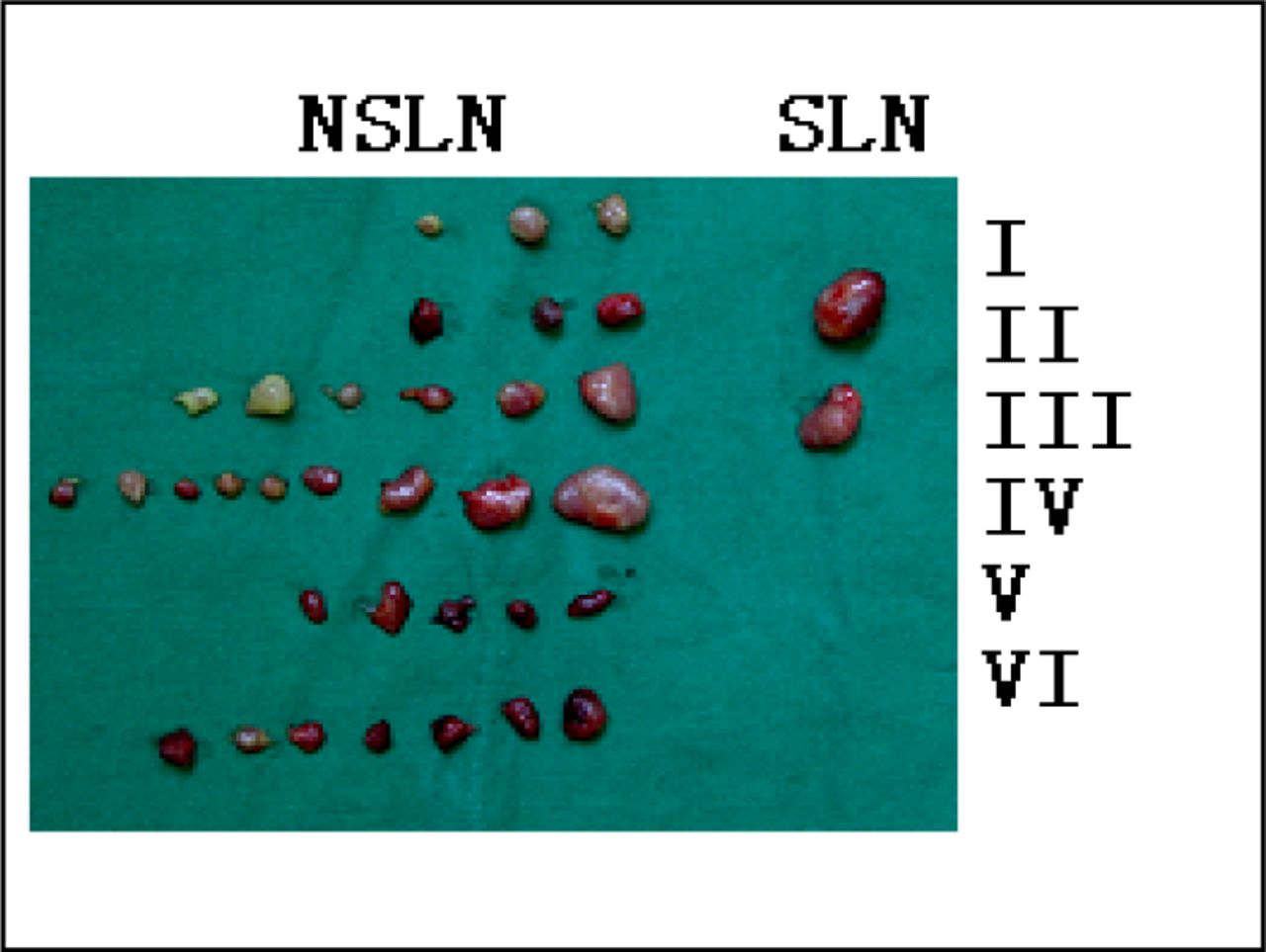
The γ-probe: A portable German CRYSTAL Probe 2000 γ-probe detector was used. At operation, the platysma muscle and sternomastoid muscle were turned over backwards and the operating field was fully exposed, with the hot points showing 3 times more radiocounting than the background (Fig.3). The operating processes were respectively recorded, according to the clinical zoning standards for lymph nodes of the neck, i.e. the rules for zones-I, II, III, IV, V and VI, instituted by the U.S. Otorhinolaryngology and Head and Neck Surgery Foundation College in 1991 (Fig.4).
The γ-probe detection for identifying the zone-III SLN of the right neck.
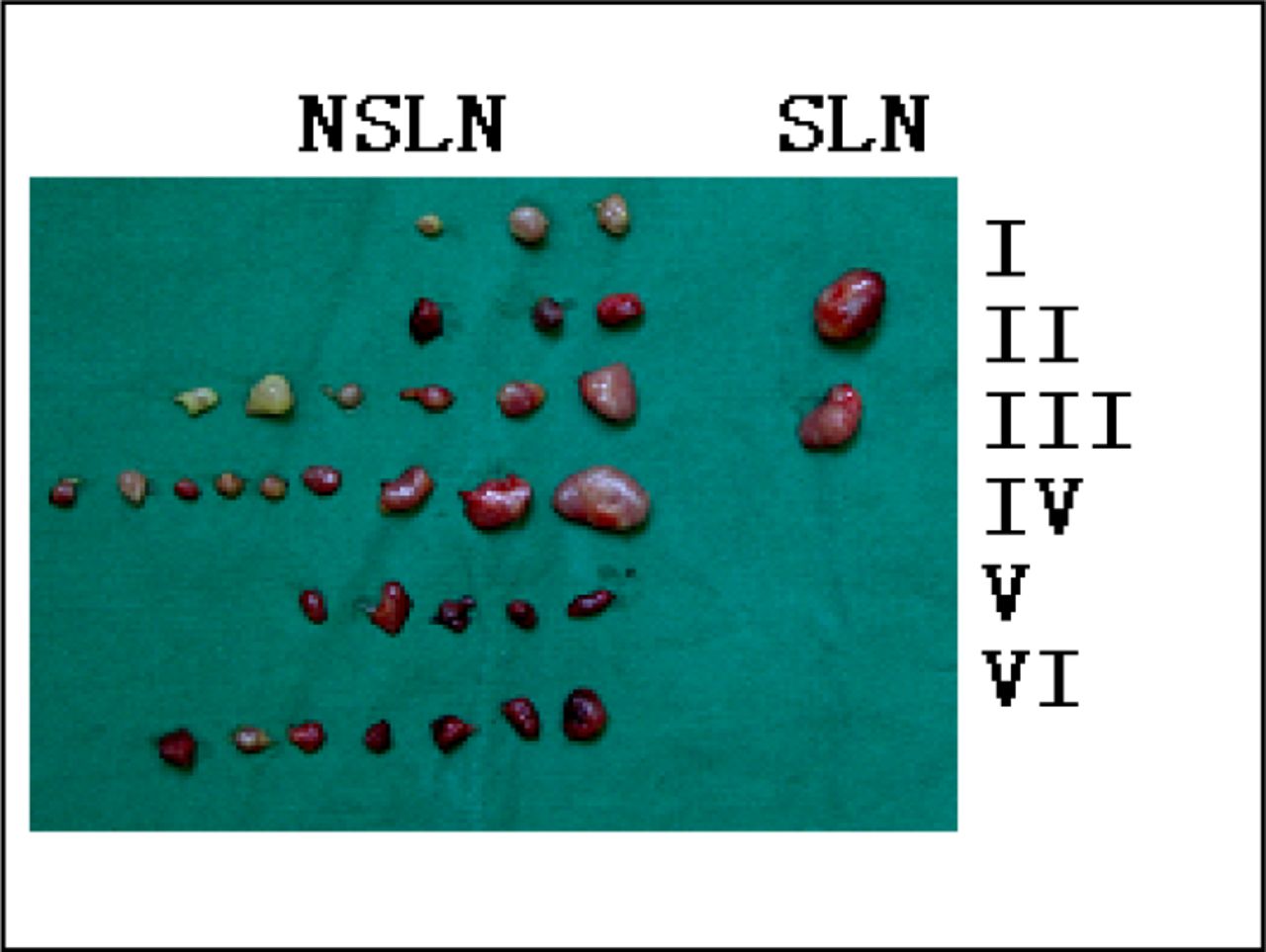
The γ-probe detection for identifying the SLN and NSLN of the patients with gingival carcinoma and its distribution.
Pathological examination of the lymph nodes
Routine section of lymph-node samples and H&E staining were conducted. Serial sections were utilized for the patients with negative results. H&E staining was performed on 10 sections, with a thickness of 4 μm and an interval of 25 μm.
Immunohistochemistry (IHC)
AE1/AE3 antibodies (mouse-antihuman keratin antibody, Beijing Zhongshan BioTech Co. Ltd.) were used to conduct the IHC as follows: After removal of the paraffin, the tissues were hydrated, washed 2 to 3 times with PBS for 5 min each time, covered with 1 to 2 drops of 3% H202 and 80% formaldehyde for 10 min at room temperature and washed as before with PBS. The samples were sealed with normal goat serum and incubated at 37°C for 20 min, followed by monoclonal antibody CK (AE1/AE3) addition and holding at 4°C overnight. After the biotin-labeled second antibody was added, the samples were maintained at 37°C for 30 min, after which an alkaline phosphatase-labeled antibiotin solution was added and held for an additional 30 min at 37°C. Color developer was applied and samples stained with H&E stain. The CK antigen was located in the cytoplasm, with the positive cells displaying a rose-pink color and the negative cells showing no pigmentation.
RESULTS
Comparison among three SLN examination methods
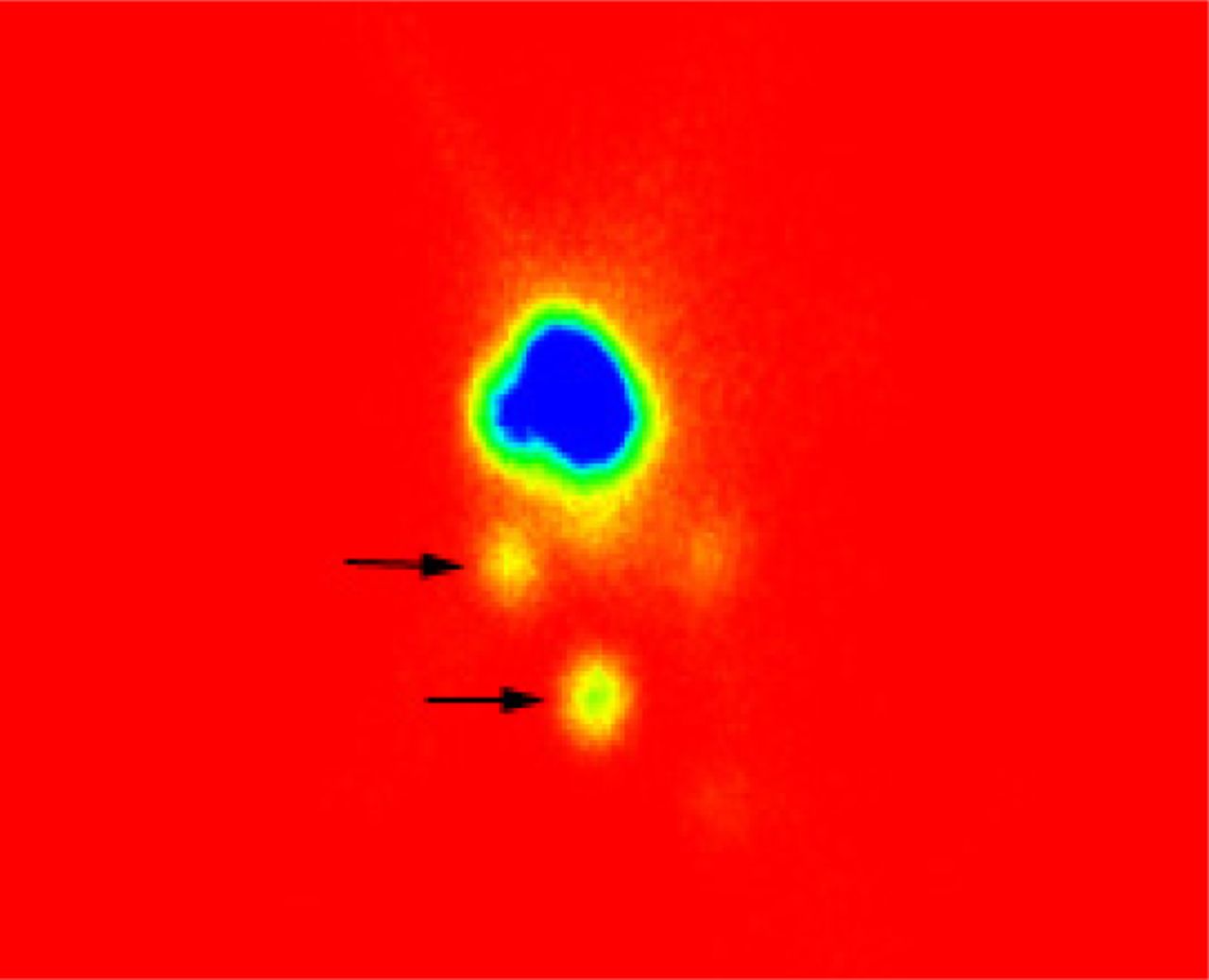
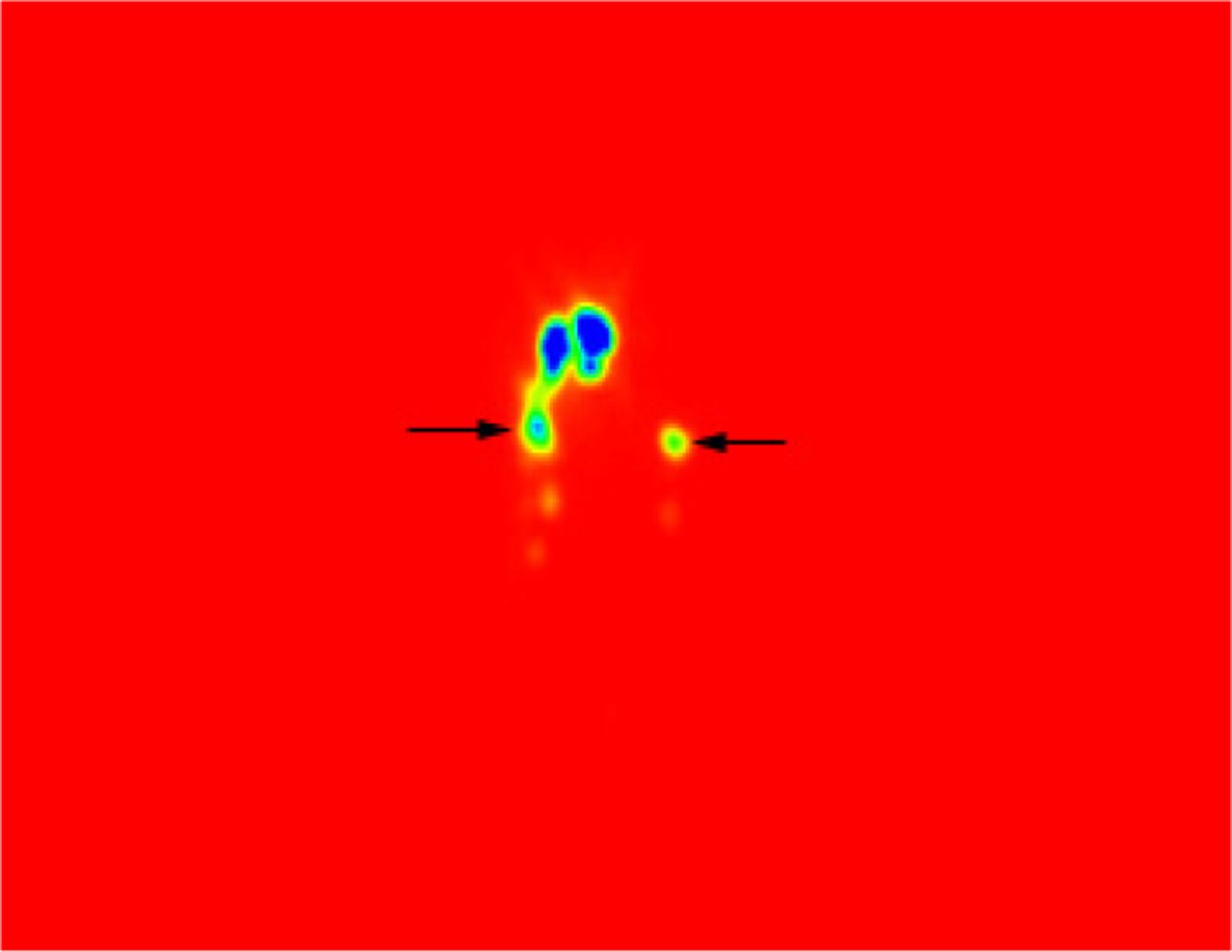
To examine the SLNs, the blue-stain, γ-probe and SPECT lymphoscintigraphy methods or tables were used respectively in 25 (80%), 31(100%) and 30 (96.5%) of the cases, resulting in a detection of 45, 55 and 51 SLNs respectively in the 3 groups, with an average of 1 to 3 in each case. The SLNs were mainly distributed in zone-I, II and III (Fig.5) and only a few in zone-IV. In this study, no SLNs were found in zone-V. The blue-stain method failed to find the SLN in zone-V. One case with contralateral lymph-node imaging was detected by SPECT lymphoscintigraphy (Fig. 6).
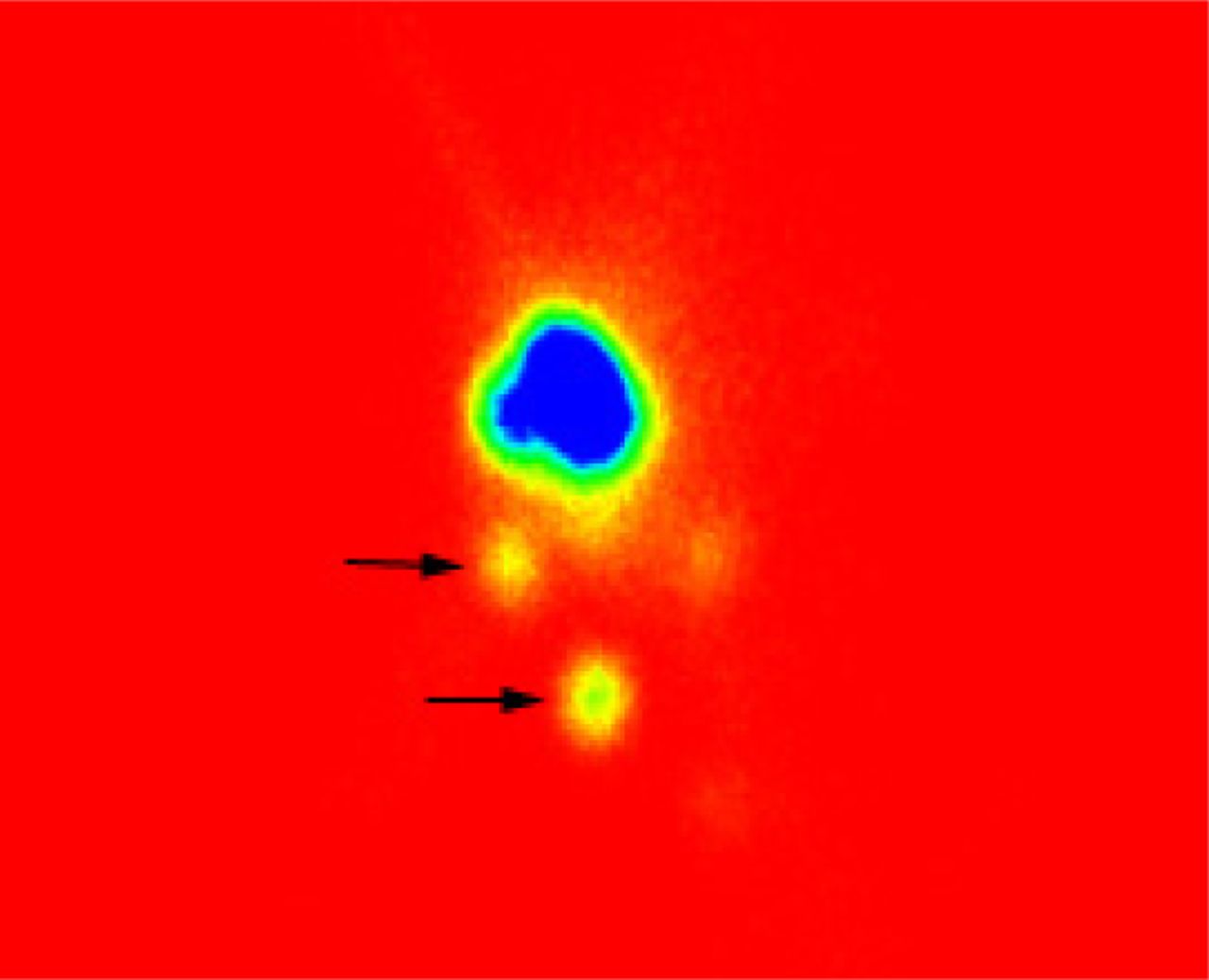
The ECT lymphoscintigraphy showed zone-I and II SLN of the left neck (left lateral position).
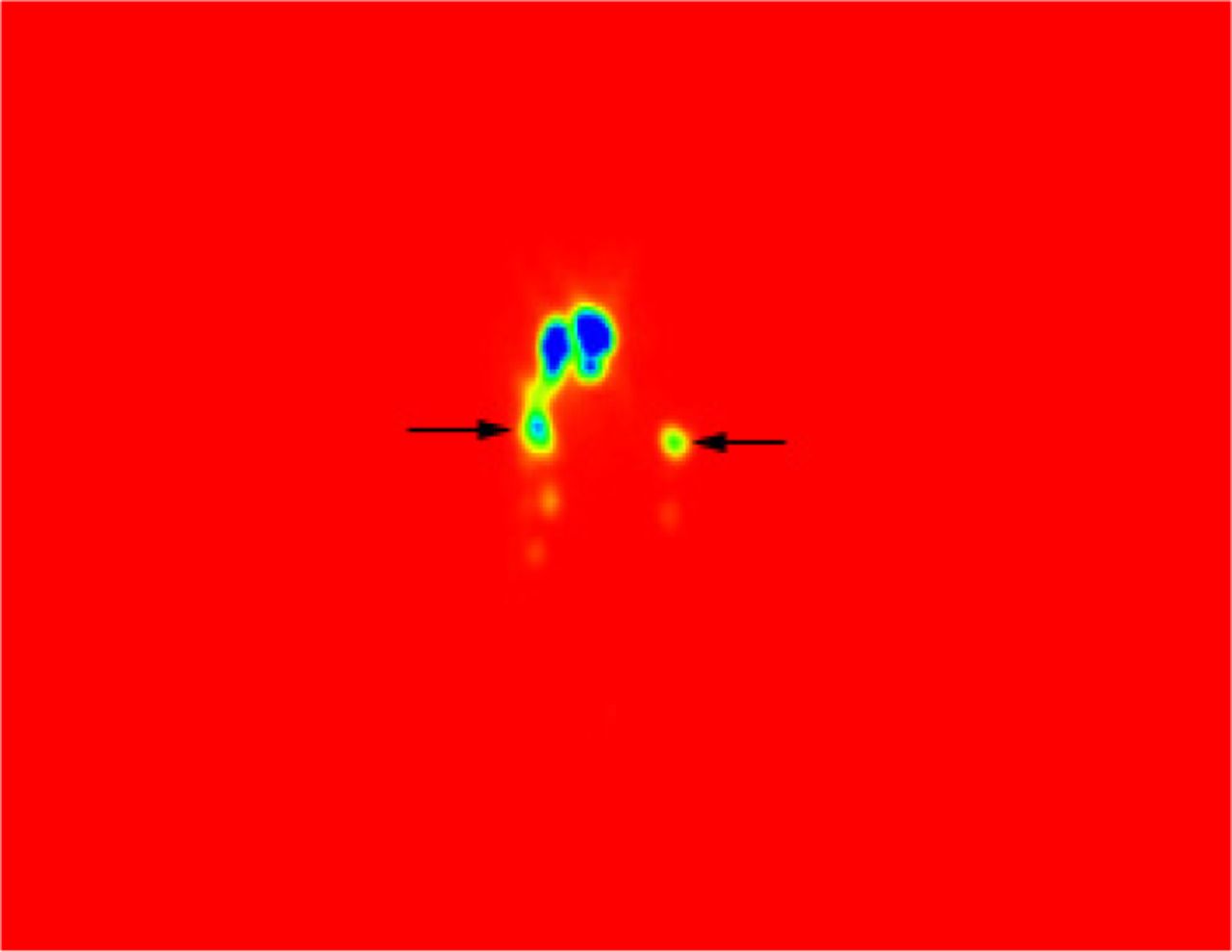
The ECT lymphoscintigraphy showed zone-II SLN of the bilateral neck (anteposition).
Evaluation of cervical lymph-node metastasis
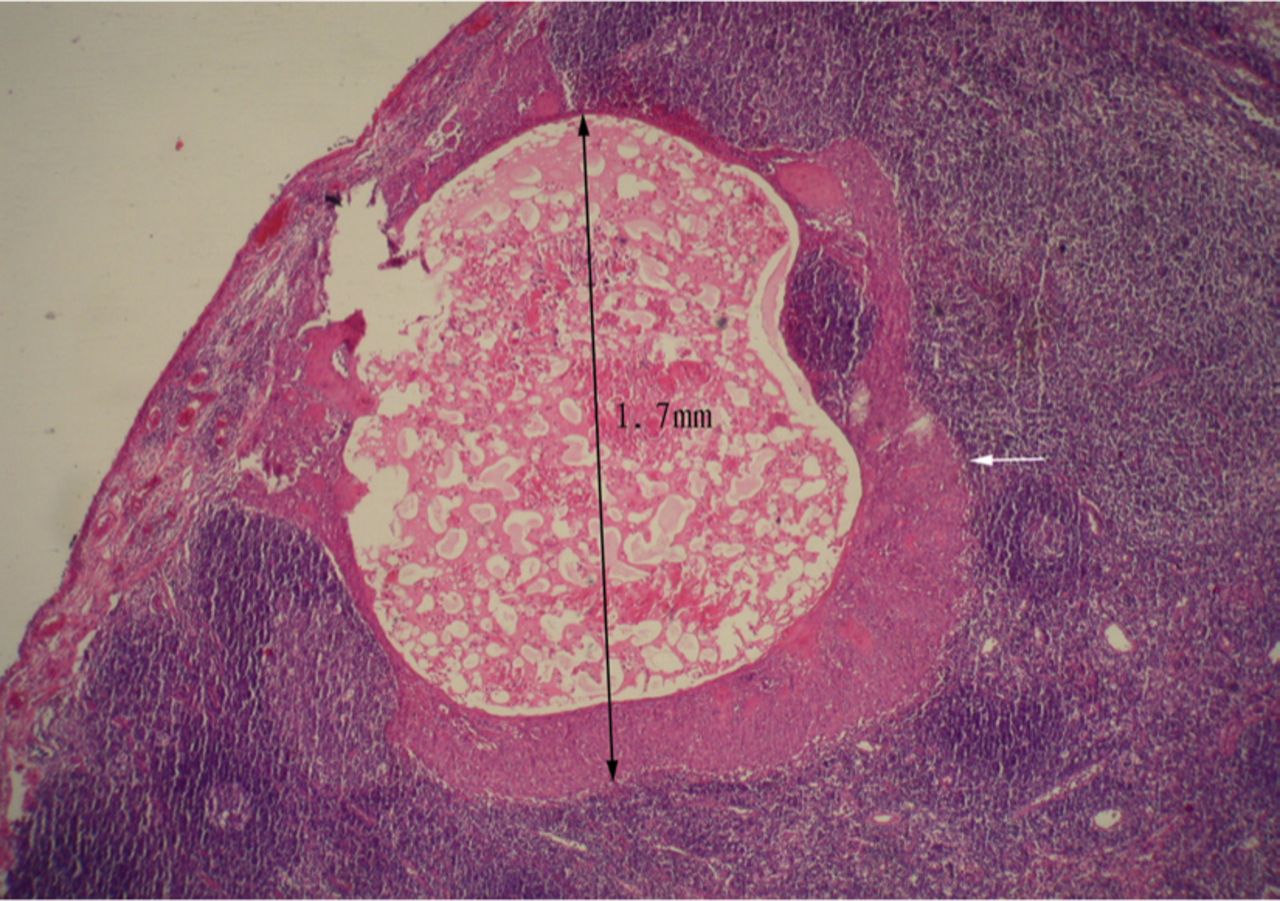
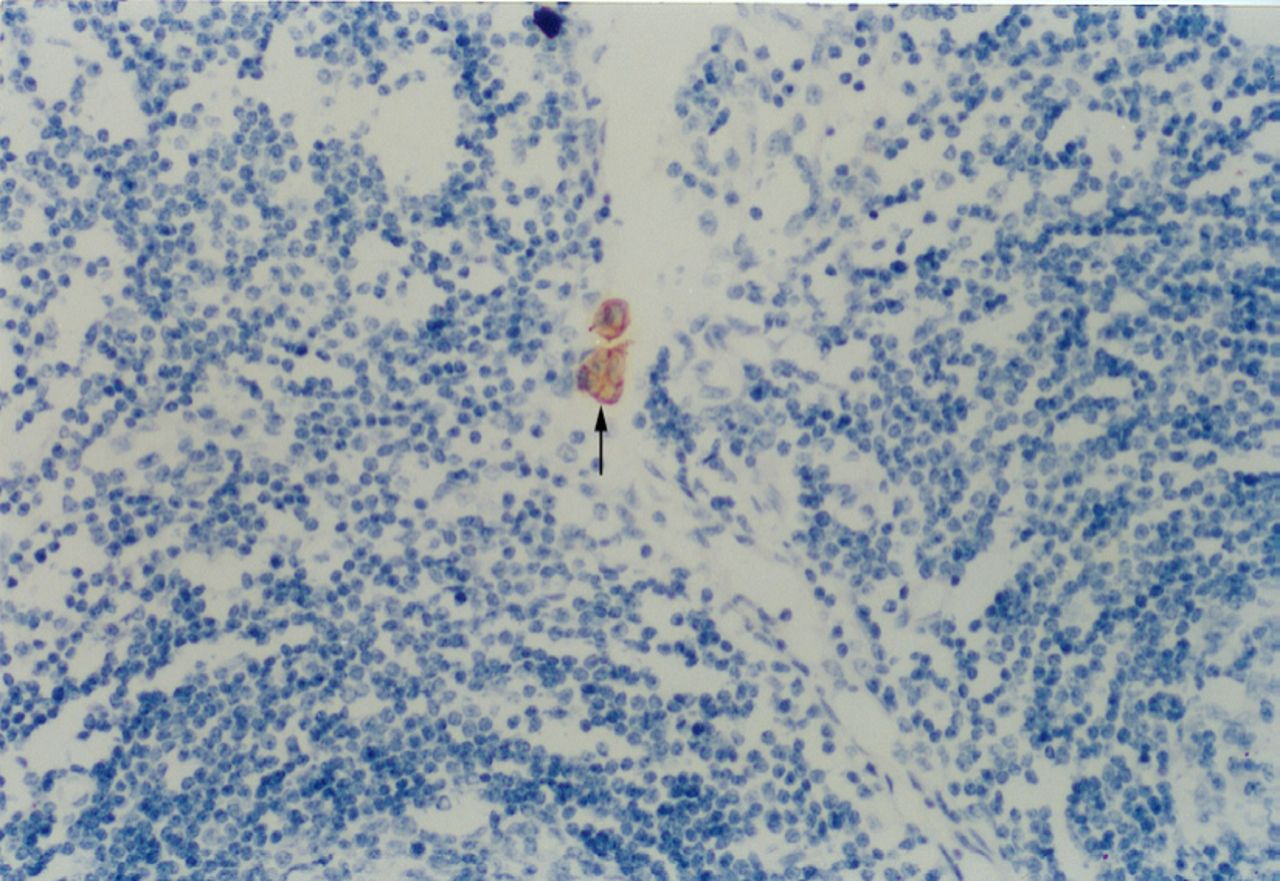
Among the 31 patients, there were 55 SLNs and 1,302 non-SLNs. Six positive metastatic SLN were detected by routine pathological examination, and one of these cases was found to have a positive metastatic non-SLN. During a routine pathological examination of the negative SLN metastasis and non-SLN, 1 positive SLN metastasis was found after an examination of serial sections plus routine H&E staining, and 2 micrometastases were detected using serial sections plus the AE3 immunohistochemical staining method (Fig.7). One of these cases showed a positive node from serial sections plus routine H&E staining and from serial sections plus AE3 IHC staining (Fig.8). Metastases of the SLN and NSLN were seen in the 9 detected nodes. Four nodes were found with a singular tumor (usually ignored by routine pathological examination) or with multiple isolated tumor cells which were located on the marginal sinus of the SLN or in the lymphatic sinuses of the nodes. There were 3 lymph nodes displaying micrometastasis, with a diameter of less than 2 mm and 2 imperceptible SLN metastases, with a diameter of more than 2 mm.
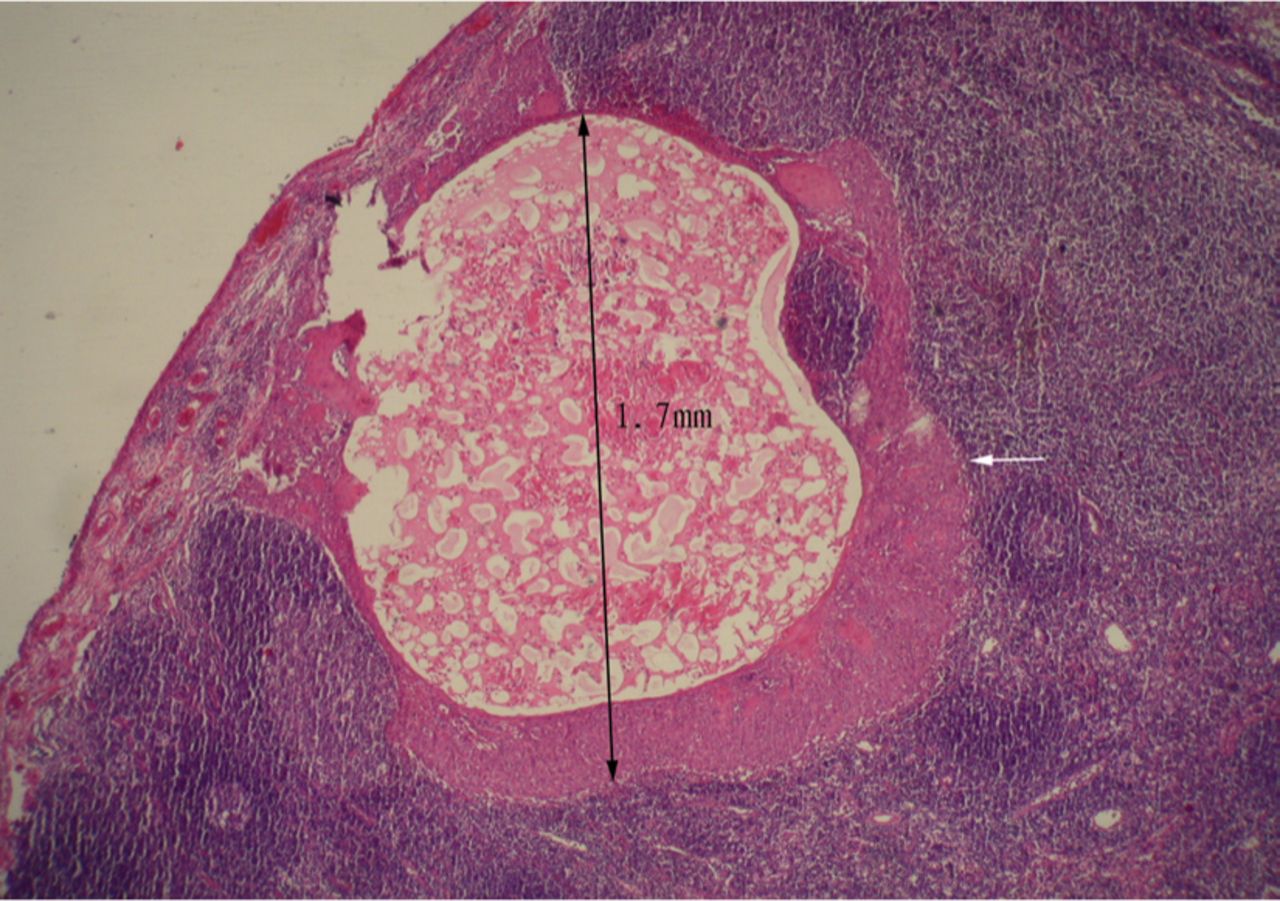
Micrometastasis (less than 2 mm) H&E×100 was shown on serial sections.
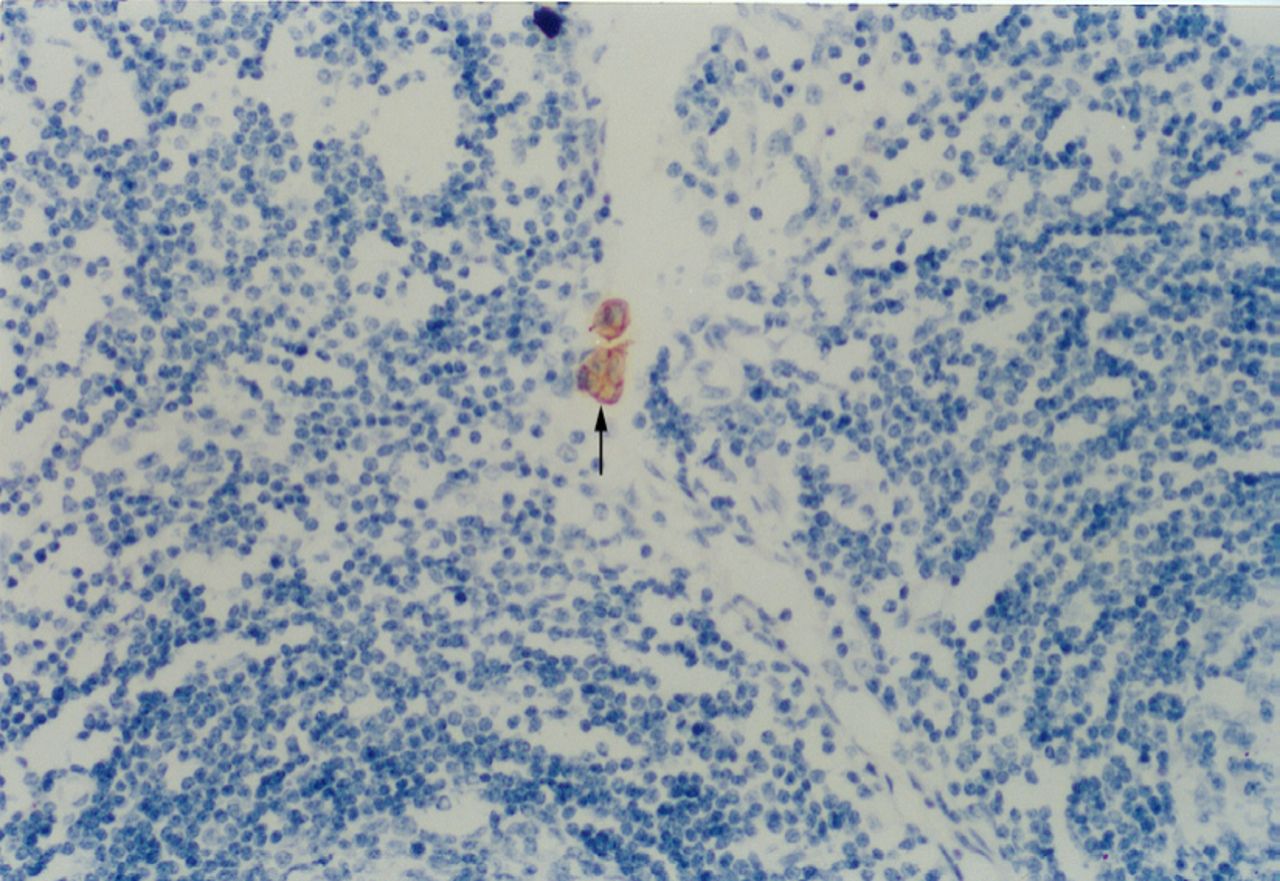
AE3 IHC stain showed a positive SLN (H&E×100).
DISCUSSION
The concept of the sentinel lymph node (SLN) was first introduced by Cabanas[2] in 1977. When he conducted a dorsum-penis lymphangiography, Cabanas found that there was a group of penile-carcinoma patients who developed early lymphatic metastases. So he named the nodes SLN, meaning the lymph node that first received lymphatic drainage from the tumor and that the tumor metastasis occurred earliest there. At the same time, he suggested that a routine sentinel lymph node biopsy (SLNB) at the bilateral inguinal groove of the penile-carcinoma patients be performed, and that the clearance of inguinal lymph nodes be conducted in the patients with positive SLNs. However, his point of view did not bring about significant widespread attention owing to a lack of the technology and general views then.
Development of head and neck microsurgery has replaced part of the traditional operating techniques, with a decrease in the patients’wound and improvement of their quality of life. Diagnosis and treatment of the cervical lymph nodes for the cases with Stage-cN0 oral carcinoma has always been difficult for maxillofacial surgeons. There has been extensive progress in medical imaging over the past years, e.g., FDG-PET has shown to be much better diagnostic value for cervical lymph-node metastases greater than 5 mm. However, a thorough diagnosis is still needed for micrometastasis of nodes of less than 5 mm because of the difficulty of discrimination[3]. SLNB has been extensively applied in tumor diagnosis and staging and producing an operation program for breast cancer and malignant melanoma, etc[4,5]. It has been emphasized in many reports that the target clearance should depend on ascertainment of lymphatic metastasis in the drainage area of Stage-cN0 oral carcinoma, and regional neck dissection has replaced radical neck dissection (RND)[6,7]. A rational decrease of the RND and its complication can be achieved. Neck dissection will not be needed if the cervical glands are negative, so a correct analysis is essential and vitally significant for planning the therapeutic regimen for Stage-cN0 OSCC patients.
In our study, the radiological lymph node imaging, portable γ–probe and blue stain were used to examine the SLN of our 31 patients. These methods were used respectively for detection of the SLN in 25 (80%), 31 (100%) and 30 (96.5%) of the cases, among which the intraoperative γ-probe detection ranked first in sensitivity. Though the sensitivity of the blue stain method was relatively lower, it is inexpensive and convenient to administer, with an easily visualized identification of the nodes[8]. Combined application of the 3 methods provides high sensitivity for examination of the SLN.
The results of our study revealed that the SLNs of Stage-cN0 OSCC were mainly situated at zone-I, II and III. The SLN at zone-IV and contralateral side only could be found in a few patients, thus forming a so-called skipped drainage[9]. The sensitivity of lymphoscintigraphy was lower compared to the γ-probe detection, but its preoperative imaging can define the position of the SLN in advance, thus avoiding omission of the contralateral draining lymph node. However, the other two methods failed to detect the contralateral lymph nodes, which caused omission of the nodes and misjudgement of the staging. It’s worth noting that during the lymphoscintigraphy, there was a great variance in the imaging time because of different varieties of the radioactive drugs (such as particle diameters). Therefore, dynamic observation was needed and if necessary, delayed imaging should be conducted[10].
In 31 patients, there were 55 SLNs and 1,302 non-SLNs. The results indicated that 6 positive metastases of the SLN were detected by routine pathological examination, among which 1 case was found with an accompanied positive metastasis of non-SLNs. No single positive metastasis was found in the non-SLN cases. Most of the lymphatic metastasis first occurred in the SLN and only a few SLN were seen in the non-SLN, thus indicating that in most instances, routine pathological sections and H&E staining of the SLN can supply accurate clinical pathologic diagnosis and tumor staging[11], and that the state of SLN can signify the lymph-node condition of most Stage-cN0 OSCC patients.
Based on an analysis from Hermanek et al.[12] and histopathological characteristics of the imperceptible lymphatic metastasis, the SLN imperceptible metastasis can be divided into three kinds, i.e., isolated tumor cells, micrometastasis with a diameter of less than 2 mm, and metastasis over 2 mm[13]. Among the three kinds, most of the isolated tumor cells were situated at the marginal sinus of the SLN or lymphatic sinuses of the lymph nodes, and it was an imperceptible metastasis that was easily missed by routine pathological examinations. Then serial sections and an IHC (AE1/AE3) assay were conducted, and 2 more positive SLN metastases were added. The result of the staging was raised up to 6.5%, so that with Stage-cN0 OSCC cases the probable micrometastases that may exist in SLN and non-SLN can be discovered with a higher accuracy. By use of routine H&E staining it was difficult to discriminate the isolated cancer cell group from the sinal histocytes and especially, the micrometastasis situated at the marginal sinus of the nodes and inside the lymphatic sinuses. IHC is helpful for detection of the micrometastasis[14]. Based on current routine pathological examinations, false negatives were found in SLNB[15]. This required the pathologists to concentrate their energy on conducting serial sections on 1 to 2 lymph nodes with a metastasis of most probability, and to complete the accurate staging of the lymph nodes, in combination with the IHC methods[16].
United application of lymphoscintigraphy, γ-probe and blue stain can enhance the high sensitivity for SLN examination. SLNB has a very high negative prediction rate, and preoperative lymphoscintigraphy may predict the exact position of SLN, so as to prevent omission of the contralateral draining lymph nodes. In most instances, routine pathological sections and H&E staining of the SLN can supply accurate clinical pathologic diagnosis and tumor staging. Micrometastases, which are difficult to detect by H&E staining of routine pathological sections, can be found by using serial sections and an IHC (AE1/AE3) analysis.
- Received January 4, 2007.
- Accepted January 23, 2007.
- Copyright © 2007 by Tianjin Medical University Cancer Institute & Hospital and Springer
In this issue






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.