

keywords
Case Report
A 36-year-old man with a neoplasm in his right-leg had undergone surgical removal of this neoplasm at an out-patient clinic (OPD). The tumor size was about 1 cm× 1 cm× 0.5 cm. It was knotty and nonencapsulated. Its cross-section was kermesinus and its texture was moderate. The pathological examination confirmed a diagnosis of Kaposiform hemangioendothelioma.
Discussion
Kaposiform haemangioendothelioma is a locally aggressive, immature vascular neoplasm, characterized by a predominant Kaposi sarcoma-like fascicular spindle cell growth pattem. It also has been called Kaposi-like infantile haemangioendothelioma, or haemangioma with Kaposi sarcoma-like features. This is a rare tumor with no known racial predilection. The tumor most commonly occurs in the retroperitoneum and the skin, but it can also occur in the head and neck region, mediastinum, and deeper soft tissues of the trunk and extremities. Kaposiform haemangioendothelioma typically occurs in infancy and first decade of life, but adult cases are increasingly recognized. Retroperitoneal tumors usually present as an abdominal mass, ascites, intestinal obstruction, and jaundice. Deep soft tissue lesions produce single or multiple masses and may involve the underlying bone and rarely regional lymph nodes (variably interpreted as either local extension or local metastasis). Cutaneous lesions present as ill defined violaceous plaques. Consumption coagulopathy (Kasabach-Merritt syndrome) may complicate the larger tumors due to activation of clotting pathways within the tumor vasculature. There is no known association with HIV infection or HHV8.
Cutaneous lesions appear as ill defined, violaceous plaques. Soft tissue tumors are grayish to reddish, multi-nodular, and may coalesce and encase surrounding structures. Microscopically, the tumor grows in the form of infiltrative vague lobules separated by fibrous septa. It consists predominantly of criss-crossing spindle cell fascicles inter-spersed with capillaries. The fascicles are curved or straight, and may be compact with few interspersed spaces or more loosely arranged, containing slit-like, sieve-like or crescent-shaped vascular lumens. Nuclear atypia and mitotic activity are usually inconspicuous. Rarely, the spindle cell fascicles may blend with round “glomeruloid solid nests of polygonal/epithelioid endothelial cells which possess abundant eosinophilic cytoplasm". The interspersed capillaries are lined by flat or plump endothelial cells, and there can be tumor lobules resembling cellular haemangioma or capillary haemangioma. There are often adjacent foci resembling lymphangiomatosis. Fibrin thrombi and fragmented red cells can be found in the slit-like spaces and the capillaries. There may be haemorrhage, haemosiderin deposition and rare hyaline globules. We noted these phenomena in our case Fig.1.

H&E staining (200 and 400x)
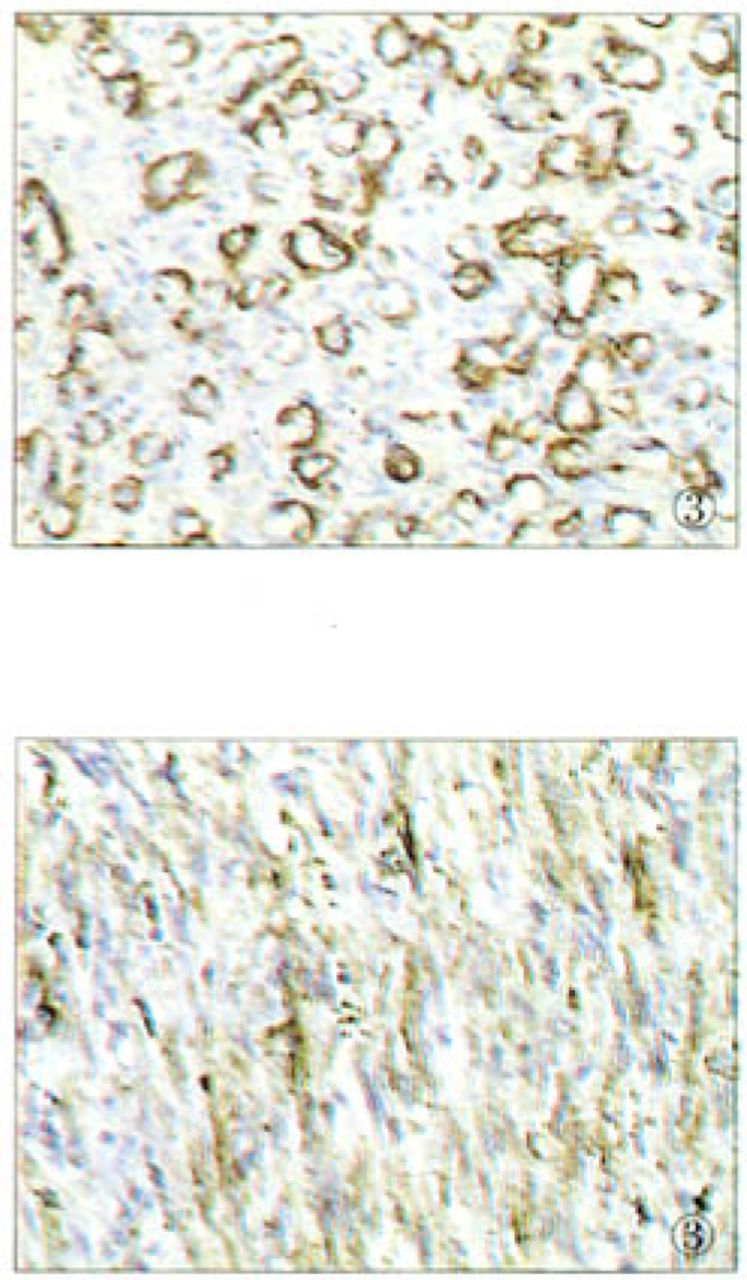
The spindle cells are usually negative for Factor VUI-related antigen, but positive for CD34 and CD 31, especially those lining vascular slits. Muscle-specific actin highlights variable numbers of spindle cells, suggesting the presence of pericytes in at least some areas. In this case, positive expression of CD34, SMA can be seen, and Factor VIII was expressed obscurely Fig.2.Fig.3. Ultrastructural hallmarks of endothelial cells are poorly developed in the spindle cells and represented by poorly formed lumens and discontinuous basal lamina. Weibel-Palade bodies may be totally absent.

Positive immunostaining of CD34 of the tumor cells (200x).

Positive immunostaining of (SMA) of the tumor cells (200* ).
Kaposiform haemangioendothelioma shows no tendency for spontaneous regression. The prognosis varies with the site and size of the lesion. Outlook is poor for large tumors occurring in infancy complicated by Kasabach-Merritt syndrome, especially when occurring in intraabdominal sites. Lesions in the somatic soft tissue are curable by complete excision, and recurrence appears to be rare.
- Received August 3, 2006.
- Accepted August 22, 2006.
- Copyright © 2006 by Tianjin Medical University Cancer Institute & Hospital and Springer
In this issue






{kind=link}
{kind=link}
{kind=link}
Related Articles
Cited By...
- No citing articles found.