

Abstract
OBJECTIVE To evaluate the feasibility of 18F-deoxyglucose positron emission tomography (18F-FDG PET) in the staging of non-small cell lung cancer (NSCLC).
METHODS 105 patients with NSCLC had been examined by 18F-FDG PET before radiotherapy. The results of the 18F-FDG PET examination were compared with those of CT.
RESULTS The staging was changed in 38 patients because of 18F-FDG PET findings, with PET resulting in upstaging in 31 patients and downstaging in seven patients. Because of distant metastasis detected by PET, 21 patients received palliative treatment. Six of the seven downstaged patients underwent radical surgery, among which the PET findings were concordant with the pathological findings in five patients. Distant metastasis detected by PET elevated the pre-PET stage: at stage I 10.0% (2/20), stage II 14.3% (3/21)and stage III 25.0%(16/64), respectively.
CONCLUSION 18F-FDG PET, by changing clinical staging in 36.2% (38/105) of NSCLC patients, has an impact on treatment strategy in NSCLC patients.
keywords
The use of 18F-deoxyglucose positron emission tomography (18F-FDG PET) has become of great importance in the diagnosis and staging of malignant tumors. In this study, in order to evaluate the value of 18F-FDG PET in the clinical staging for non-small cell lung cancer (NSCLC), we retrospectively analysed the 18F-FDG PET results of 105 NSCLC patients.
Materials and Methods
Clinical data
From June 2001 to January 2003, 105 NSCLC patients who were going to receive radical surgery in the PET-CT Center of Shandong Tumor Hospital and PET Center of Wanjie Hospital Zibo Shandong, were included in our study. There were 71 males and 34 females, with ages of 25 to 80 years and an average age of 55.3 years. All the patient pathology had been verified by cytological or pathological examination. The tumors included 58 squamous cell carcinomas, 40 adenocarcinomas, three alveolar cell carcinomas and four adenosquamous carcinomas. Enhanced CT in the thorax and epigastrium, abdominal B-mode ultrasound and bone scintigraphy were applied in these patients to determine the clinical staging: All of these patients had 3-24 months of follow-up.
Examination method
18F-FDG was automatically synthesized by a cyclotron GE Minitrace with a radiochemical purity > 95%. The instruments employed were a GE whole body advanced PET scanner and a GE discovery LS PET-CT system with a resolution of 5 mm. All of the patients fasted for 6-8 h before examination and were injected with 18F-FDG (185-370 MBq) via a cubital vein 50 min before emission and transmission scanning. When the examination began the patient was in a supine position and the aquisition time was 10 min per axial field of view (AFOV). The enumeration per transaxial image in emission scanning was at least 1.2 × 107, while that was at least 1 × 108 in transmission scanning, and 6 AFOV (86.7 cm) were aquired. After the scanning images were reconstructed, 35 transaxial images with 4.25 mm thickness were obtained, and then they were reconstructed and progressed to coronal and sagittal images which were analyzed by macroscopy or by a semi-quantitative method.
Analysis of results
Quantitative analysis
Two experienced PET diagnosticians interpreted the PET scans simultaneously, one of whom knew nothing about the other clinical data from the patient. The areas in which accumulations were greater than that in the surrounding normal tissues were considered malignant lesions, while the areas of accumulations slightly higher than, equal to, or lower than the surrounding normal tissues would be considered to be non-tumor lesions.
Semi-quantitative analysis
The standard uptake value (SUV) was the ratio of the FDG uptake value (kBq) in unit weight tissue to the FDG injection dose in unit body weight (g). The method of calculating the FDG uptake value in the unit weight tissue was as follows: The patients' body weight (g) and FDG injection dose were known. Then the 1.2 cm2 small area of interest (ROI) was located in the region with the maximal FDG uptake value, so the uptake value could be obtained based on the detecting efficacy of the PET imaging system. The lesion was considered malignant if the SUV obtained was greater than 2.5.
The criterion of staging
Based on the 1997 revised UICC staging, pre-PET staging was performed according to the clinical data consisting of clinical examination, radiological examination and bronchoscopic examination etc. The definition of metastasis was that the minimal cross-sectional diameter of the mediastinal and pulmonary hilar lymph nodes (LNs) were greater than 1 cm in CT scans.[1] PET staging followed the PET scanning of each patient.
Statistical analysis
The data were statistically analyzed by SPSS 10.0 and the paired t-test for dependent samples was wsed.
Results
The impact of 18F-FDG PET on clinical staging of the NSCLC patients
PET scanning changed the clinical staging in 38 NSCLC cases, including 31 upstaged cases and seven downstaged cases; the specific changes in staging are listed in Table 1. Because of distant metastasis detected by PET, 21 patients received palliative treatment in replacement for radical therapy. Because of the downstaging after PET, six patients underwent radical surgery. The staging by CT, PET and pathology in these patients can be seen in Table 2. Of the six patients, the pathological T staging in five cases was in accordance with the preoperative PET T staging; the remaining one patient staged in N1 by CT was confirmed to be a false negative (NO) by PET.
The impact of 18F-FDG PET on T staging of the NSCLC patients
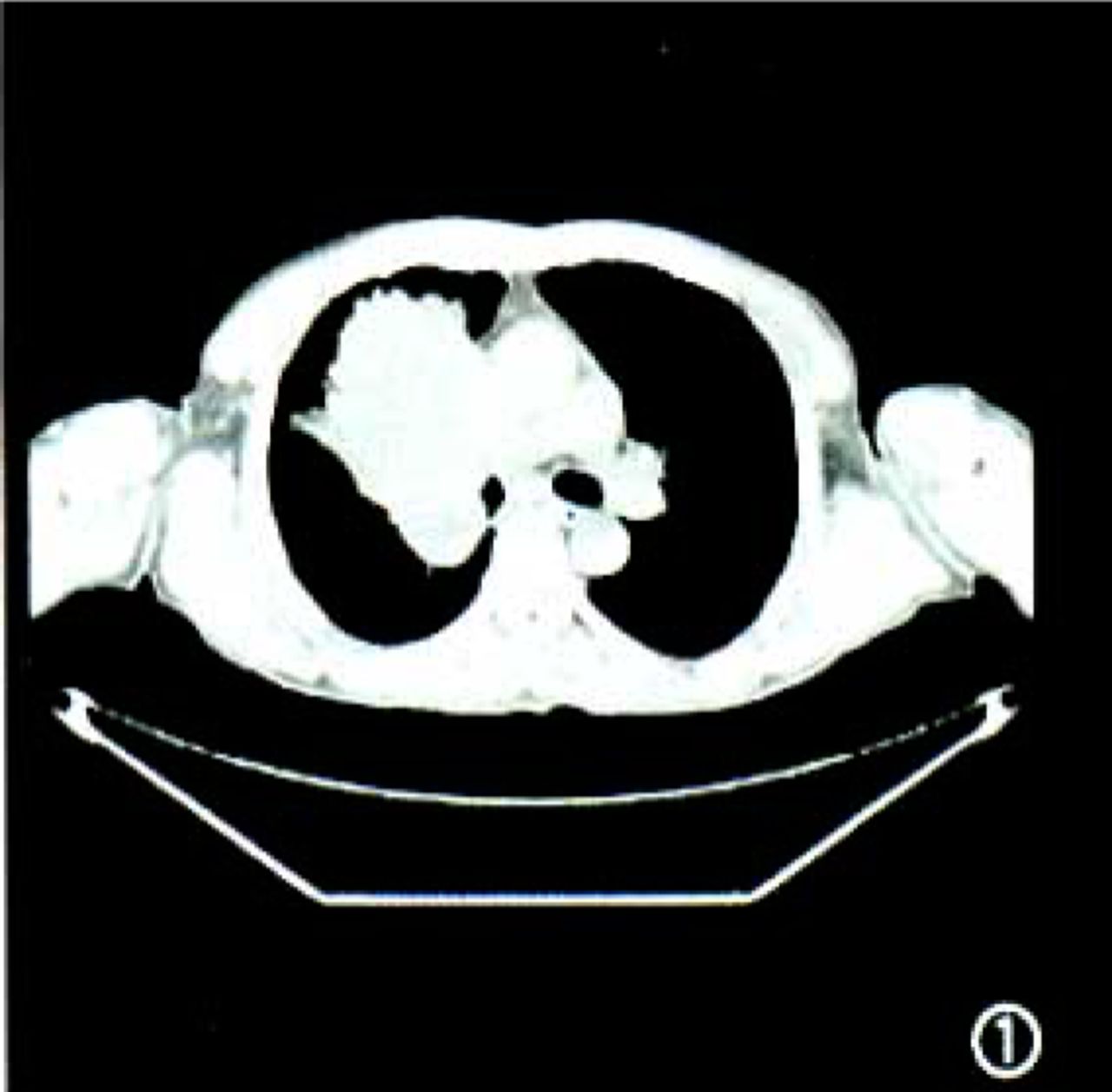
In these 105 NSCLC patients, the T staging by scanning with PET, compared to that of CT, changed in six patients consisting of four cases upstaged from T1 to T2 and two cases downstaged from T2 to Tl. In these 6 cases, there was no significant difference in the maximal cross-sectional diameter between the CT and PET image (t=1.313, P=0.246). CT could not distinguish the tumors from atelectatic tissues in 12 patients with atelectasis; but their PET scans could show clearly the margin of the tumor in nine cases. There was a significant difference in the three-dimensional cross-sections between CT and PET scans (P < 0.01,Table 3). The CT and PET scans of the typical cases are seen in (Fig.1–3.

Male, 56 years, central SCC in the right lung. CT scan showed a giant neoplasm in the right hilus..

PET scan showed that the areas, in which the FDG uptake greater, was obviously smaller than that in CT scans..
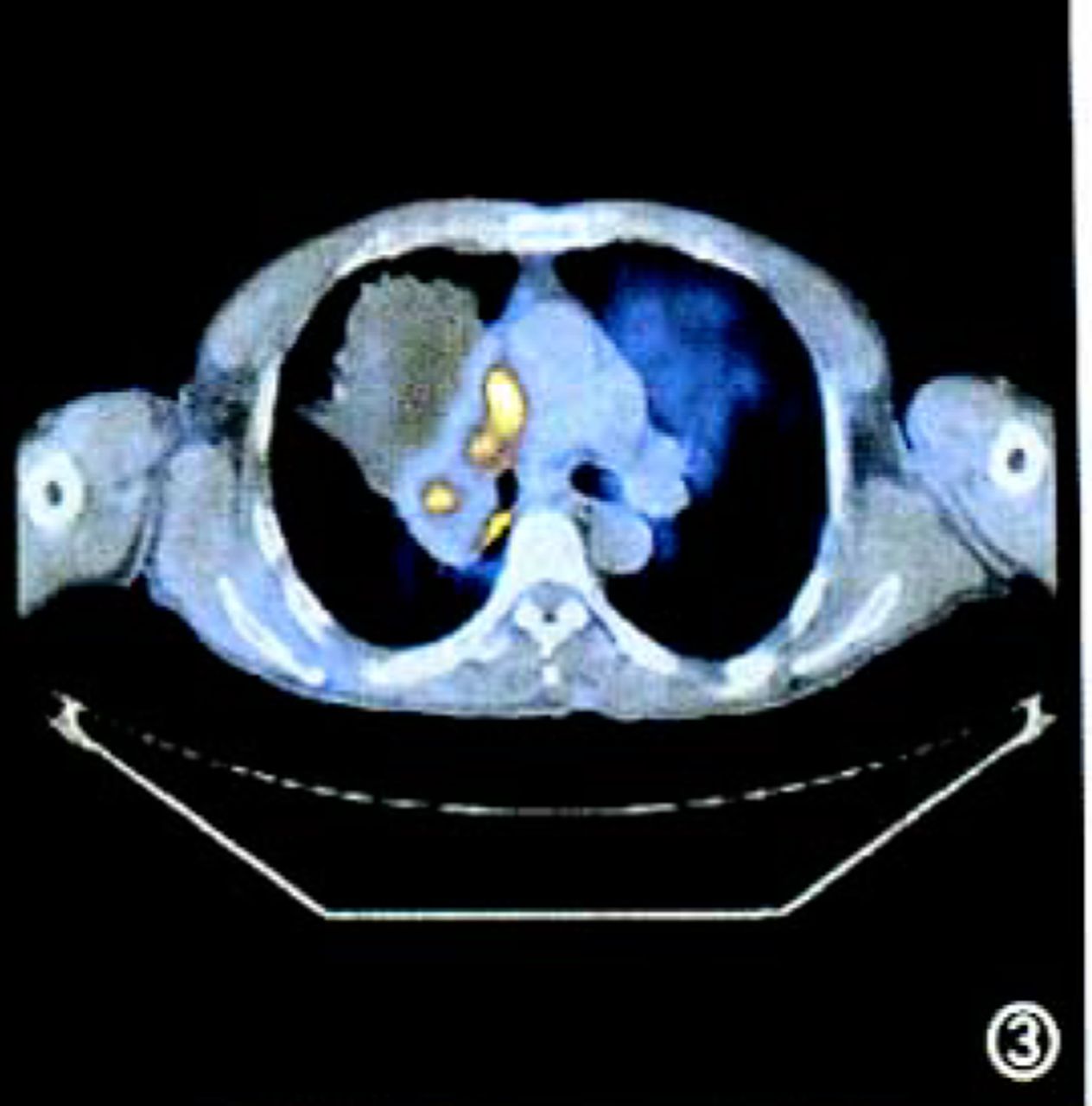
The fused PET-CT image showed extensive atelectasis in the periphery of the high metabolic region..
The impact of 18F-FDG PET on N staging of the NSCLC patients
Of the 105 NSCLC patients, the N staging of 24 patients changed, which included 18 upstaged cases (four cases from NO to N2, 1 case from NO to N3, five cases from N1 to N2, one case from N1 to N3 and seven cases from N2 to N3) and 6 downstaged cases (three cases from N2 to NO and three cases from N1 to NO).
The impact of 18F-FDG PET on M staging of the NSCLC patients
Twenty-one out of 105 NSCLC patients were detected to have having distant metastases by PET. These were not previously detected by CT, so their staging were upstaged to IV. There was on case in IIa (1/8), two cases in IIb (2/13), seven cases in IIIa (7/38) and nine cases in IIIb (9/26). A total of 24 distant metastatic foci were detected, consisting of seven foci in the lungs, three in the adrenal glands, three in the liver, four in bone, six in the abdomen and one in the brain. Following the conformal radiotherapy for three months, the three adrenal gland metastases received a second PET scanning. The results indicated that FDG uptake had decreased and the SUVs had diminished from 5.0, 9.0, 11.0 to 2.0, 3.0 and 3.5 respectively. Pain of four bone metastatic patients was relieved after radiotherapy. Clinical follow-up indicated that, two pulmonary metastases were founed to be false poritives and their PET scans showed small nodular concentrated foci with SUVs of 3.0 and 4.0 respectively. At a one year follow-up there were no metastatic symptoms in their CT scans, so the two metastatic foci were considered to be old tuberculomas; the remaining 15 foci were confirmed metastases through radiological and clinical follow-up during 3-24 months. The accuracy of PET in the detection of distant metastases was 10.0% (2/20) in stage I, 14.3% (3/21) in stage II and 25.0% (16/64) in stage III, demoustrating that the accuracy in stage III was higher than that in stages I and II.
Discussion
The impact of 18F-FDG PET on T staging in the NSCLC patients
The results of our study revealed that there was no significant difference in the T staging of NSCLC patients between PET and CT scans, while the PET scan was usefull to define the margin of tumors in NSCLC patients with atelectasis. CT scans had a favorable spatial resolution in diagnosing lung cancers and could provide the precise anatomic sites of lesions and their relationship with the important anatomic structures such as the trachea, bronchus and vessels. Because the essential factors in determining the T staging of NSCLC patients were the tumor size, the anatomic sites and the relation with the surrounding tissues, CTs played a pivotal role in defining the T stage. PET had some disadvantages of low spatial resolution, the limitation for displaying the tissue structure and the imprecise localization for lesions. Therefore PET usually failed to influence T staging of the NSCLC patients.[2]
For the patients with obstructive pneumonia, atelectasis and hydrothorax, CT had some difficulty in defining the margin of the tumors. Nonetheless, PET could discriminate between the neoplastic tissues and atelectasis. [3] The PET scans of nine cases in 12 patients with atelectasis showed the tumor margin clearly due to the significantly increased FDG uptake in the primary neoplastic tissue and the absence of FDG uptake or the slightly increased FDG uptake in the surrounding atelectatic tissue. This is helpful for contouring precisely the targets of radiotherapy, and then to lessen the radioactive injury in the surrounding normal tissue and improve the therapeutic accuracy.
In the study by Balogh et al.[4] ten NSCLC patients with obstructive pneumonitis and/or atelectasis underwent CT and PET-CT scanning, and the radiation oncologist defined two gross tumor volumes (GTV) in CT scans, that is GTVCT and GTVPET-CT; in CT scans the GTVPET-CT could further define the tumor margin to avoid obstructive pneumonitis or atelectasis, so this reduced the GTV in 50% of the patients because of the avoidance of obstructive pneumonitis or atelectasis or atelectasis mistaken for a tumor in the CT.
The impact of 18F-FDG PET on N staging in the NSCLC patients
The N staging changed in 24 out of 105 cases, with 18 cases being upgraded and six being downgraded. In six patients receiving a surgical operation, the pathological staging was in accordance with PET staging in five cases, and the PET diagnosis was a false negative in the remaining one case, namely, the N1 by CT was misdiagnosed as NO by PET. The phenomenon was induced by the intense conjunction between the metastatic lymph nodes and the primary foci, and the failure of PET to localize precisely the lesions. The fusion of CT-PET images may diminish the incidence rate of false negatives induced by the incapability of PET in diagnosing the hilus and its adjacent anatomic sites. CT has been the most non-traumatic method to evaluate mediastinal LNs in NSCLC patients for many years. The size of the LNs was utilized to estimate LN metastasis in CT scans and its minimal diameter >1 cm was considered as the criterion for metastasis. But the postoperative pathological results verified that in the diagnosis of about 30%-40% of the LNs accorded with this criterion, the enlarged LNs may be not metastatic and the metastatic LNs may be not enlarged.[5]
Some studies have shown that taking advantage of the extent of FDG uptake to stage the mediastinal LNs by the metabolic state was more precise than CT. In the study by Vansteenkiste et al., [6] pathological staging was performed in 6% of the LNs in 68 NSCLC patients and their findings compared to the CT and PET findings. The results showed that by using CT the tumors were staged correctly for 40 patients (59%) and by PET for 59 patients (87%) (P=0.0004). Of 690 LNs, PET accurately evaluated 22 metastatic LNs that were diagnosed as normal by CT and excluded 25 LNs that were diagnosed metastaticly enlarged LNs by CT. By having the ability to detect lymph nodes with a diameter 1cm, the detectable rate of PET was greater than CT.
The impact of 18F-FDG PET on M staging in the NSCLC patients
18F-FDG PET is also valuable for detection of the pulmonary foci and distant metastatic foci at other sites in NSCLC patients. In our study, PET detected 24 distant metastatic foci which had failed to be detected by CT in the 105 patients. In addition, 21 patients were upstaged to IV in clinical staging. Although 18F-FDG PET-scanning is an effective means to distinguish benign from malignant neoplasms in lungs, using the SUV cut-off level (2.5) as the discriminative criterion has not been presently established. This is due to the finding that there is some overlap between the SUV of malignant lesions with that of benign in spite of the greater SUV in malignant lesions compared to benign. Because of the increased FDG uptake in tuberculomas, the two pulmonary metastatic foci, which were tuberculomas in fact, were diagnosed by PET as false positive. We concluded, from our study, the accuracy of PET in the detection of distant metastatic foci improved as the stage increased compared to pre PET scanning, and it was 10.0% in stage I, 14.3% in II and 25.0% in III. Part of the data of the NSCLC patients in stage I and II revealed that the concordance between PET and pathological staging was 83%-87%, and concluded that a preoperative PET examination could exclude part of the patients from nonessential thoracotomy.[6,7] For most of the NSCLC patients, who needed to receive radical radiotherapy and chemotherapy failed to tolerate an operation, and whose lesions could not be resected, the pathological, staging was very difficult to obtain. Therefore patients in stage III had a greater possibility of having metastases compared to patients in stage I and II, and the accuracy of PET detecting distant metastatic foci in patients with no symptoms was greater.
In conclusion, 18F-FDG PET can reflect the metabolic state of NSCLC tumor tissues and is considered to be an improved functional radiological technique. The application of PET can change the staging of some NSCLC patients and thereby influence the therapeutic strategy and prognosis. Although PET has superiority in qualititatively indentifing the tumors, it has some false positives and false negatives. The development of a fused PET-CT imaging technique and the exploitation of new tracer agents would decrease the incidence of the false positives and the false negatives and thereby increase diagnostic accuracy.[8]
- Received December 6, 2004.
- Accepted March 3, 2005.
- Copyright © 2005 by Tianjin Medical University Cancer Institute & Hospital and Springer
In this issue






{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.