

Abstract
OBJECTIVE CT scans have become a conventional examination for hepatocellular carcinoma. Computed tomography arteriography (CTA) and computed tomography arterial portography (CTAP) are more sensitive. In this investigation, we defined the optimal time of CTA and CTAP during a dynamic scan.
METHODS CTAP: a 5-F Yashiro catheter was inserted to the superior mesentery artery under DSA, and the whole liver scanned 6 s after contrast medium injection. CTA: the 5-F Yashiro was inserted to the proper hepatic artery and a scan of the whole liver was performed 6-8s after contrast medium injection.
RESULTS In CTA, the contrast between enhancement of liver cancer and the normal liver tissue reached a peak after the contrast medium had been injected for 6~8 s. The focus was concealed by non-pathological enhancement in three cases. When the scan was delayed to 30 s after injection, the lesion could be detected clearly (P <0.05). The contrast of the image was not as good as 60~ 180 s after injection, and pathological enhancement also was not found (P >0.05). During CTAP, the frequency of an abnorminal non-perfusion area was 19.0% (4/21) at 6-8 s after injection; the contrast of low-perfusion focus and the normal liver was evident and the lesion could be detected clearly (P <0.01). The contrast was decreased at 120-180 s after injection and the image was not as clear (P >0.05).
CONCLUSION CTA and CATP are effective techniques to detect small hepatocellular carcinoma, to define the position of lesions and to estimate the feasibility of resection.
keywords
The diagnosis of primary hepatocellular carcinoma mainly depends on the clinical manifestations, AFP and the correlative imaging characteristics. CT scans have become a conventional technique for examination of hepatocellular carcinoma pre- and post-operation. However, regular CT scans have shown to be less sensitive to small lesions compared to compute tomography arteriography (CTA) and computed tomography arterial portography (CTAP).[1] This investigation was designed to define the best time to scan after injection of the contrast medium during CTA and CTAP during the dynamic scan.
Materials and Methods
Patients
There were 21 cases in this series, including patients who were under suspicion of primary hepatocellular carcinoma or who had a recurrence within the liver post-operation or who were examined after treatment in our department between March 1997 and November 2000. All the patients were males, aged from 29 to 57 years (median age of 45.5), without obvious jaundice or ascites. Hepatic function tests were in the normal range although six patients had hepatocirrhosis and splenomegaly. Of 15 patients with a significantly high AFP level, seven cases showed a negative result in regular enhanced hepatic CT scans, and four cases that were examined by an ultrasonic scan showed negative results. Three patients with hepatocellular carcinoma were surgically operated, and another three patients were found to have re-elevated AFP levels after transcatheter arterial chemoembolization (TACE). All 21 patients were examined with CTA and CTAP. No patients were found to have metastasis by chest roentgenograpy and pelvis ultrasonograpy.
Equipment
A PICKY CT-TWIN flash was used, with 120KV, 266MAS, 8~10 mm each layer, pitch 1. High-pressure automatic injector (Medrad Company, America, R16R) and DSA (Toshiba, BLA-800A) were employed for the examinations.
Methods
All patients were routinely fasted for 2~3 h before examination. CTAP was implemented first. Briefly, following routine sterilization and surgical draping,a 5-F Yashiro catheter was transluminally percutaneously intubated using a DSA machine, which was inserted into the superior mesentery artery. Then, 20~30 ml of contrast agent was injected through a high-pressure automatic injector at 3.0~3.5 ml/s. The whole liver was sequence-scanned 6 s later. For CTA: the 5-F Yashiro catheter was introduced into the hepatic artery, followed by injection of 15~20 ml contrast agent at 3.5~4.0 ml/s. The sequence-scan of the whole liver was performed 6~8 s later.
RESULTS
All 21 patients were found to have focal lesions in the liver after CTA and CTAP with diameters between 1.0~3.5 cm. Fifteen cases were diagnosed as primary carcinoma of the liver which was coincident to the results which were found after treatment. Three cases were post-operative patients with primary carcinoma of the liver, in which two cases with a new focus within the liver and one case with a local recurrence. Other cases were discovered to have a new focus within the liver after TACE.
The contrast between enhancement of liver cancer and the normal liver tissue may reach a peak at 6~8 s following injection of the contrast agent during CTA. However, the lesions were concealed by non-pathological enhancement in three cases (the proportion of non-pathological enhancement is 3/21, that is 14.3% ), in which the extension, size and number of lesions were difficult to be distinguished from non-pathological enhancement. The lesions were detected clearly when the scan was delayed to 30 s after injection, in which the contrast of enhancement of the lesions and normal liver tissue was significant (t test, P<0.05). Thus, the proper time to detect the lesions was 6~30 s after injection. The contrast of the image was not as good at 60~180 s after injection, and pathological enhancement was not found (Table l).
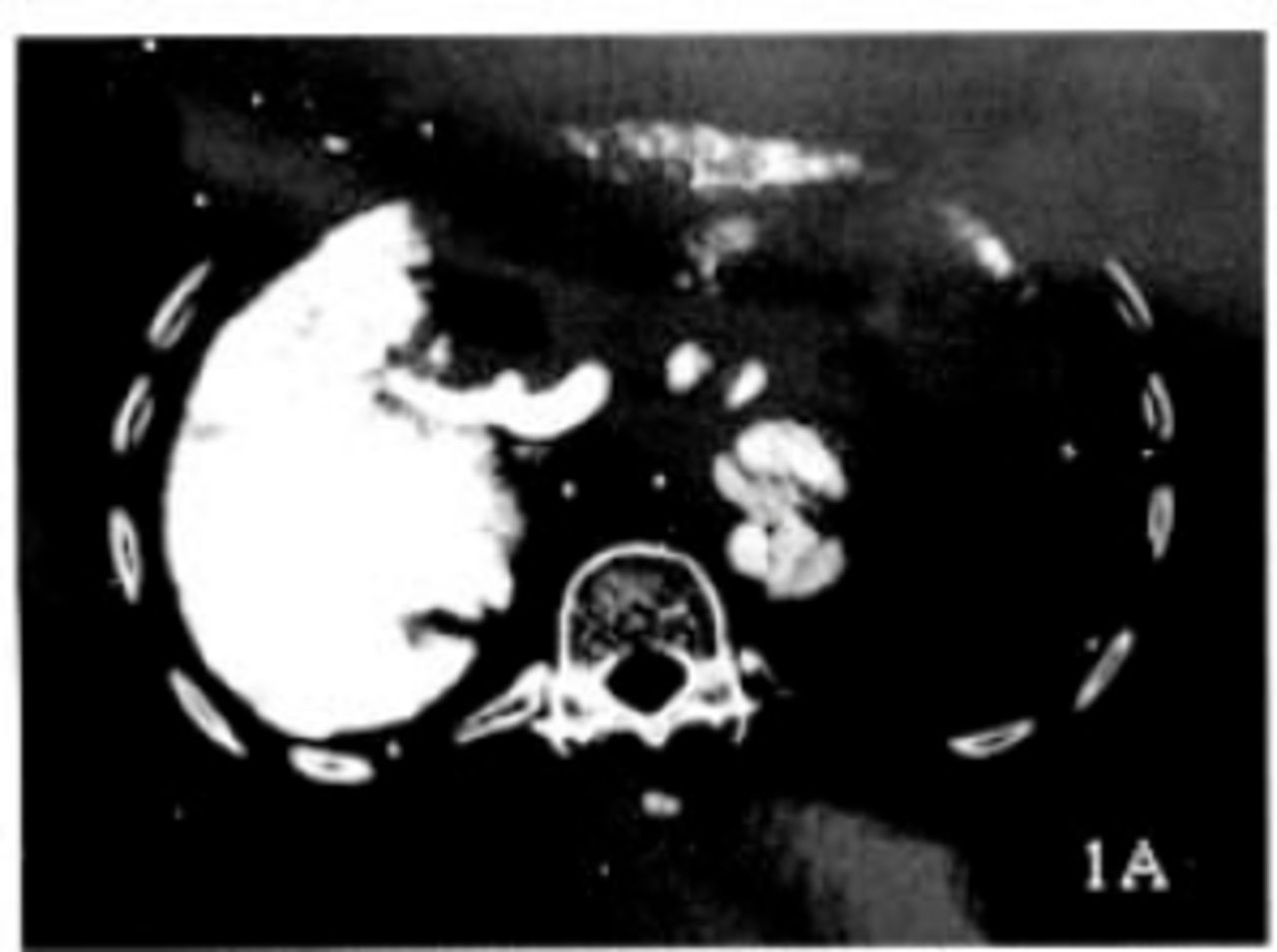
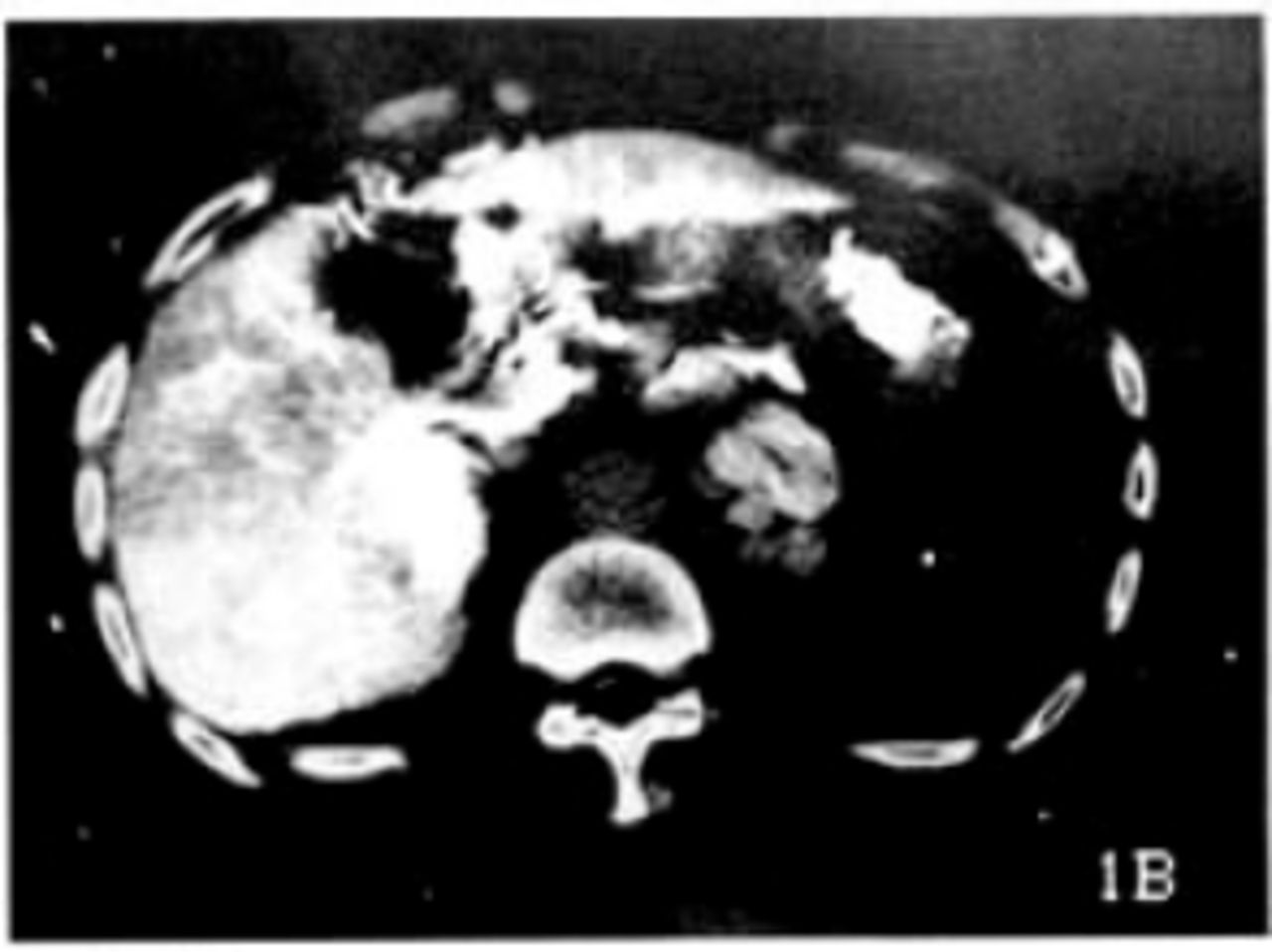
During CTAP, the frequency of erose or cuneate exceptional non-perfusion area was 19.0% (4/21) 6~8 s after injection (Fig.1). The contrast of low-perfusion focus and normal liver was apparent after 30~60 s, and the lesions could be detected clearly (t test, P< 0.01), while the contrast became indistinguishable at 120-180 s after injection, and the image was not as clear (t test, P> 0.05)(Table 1).
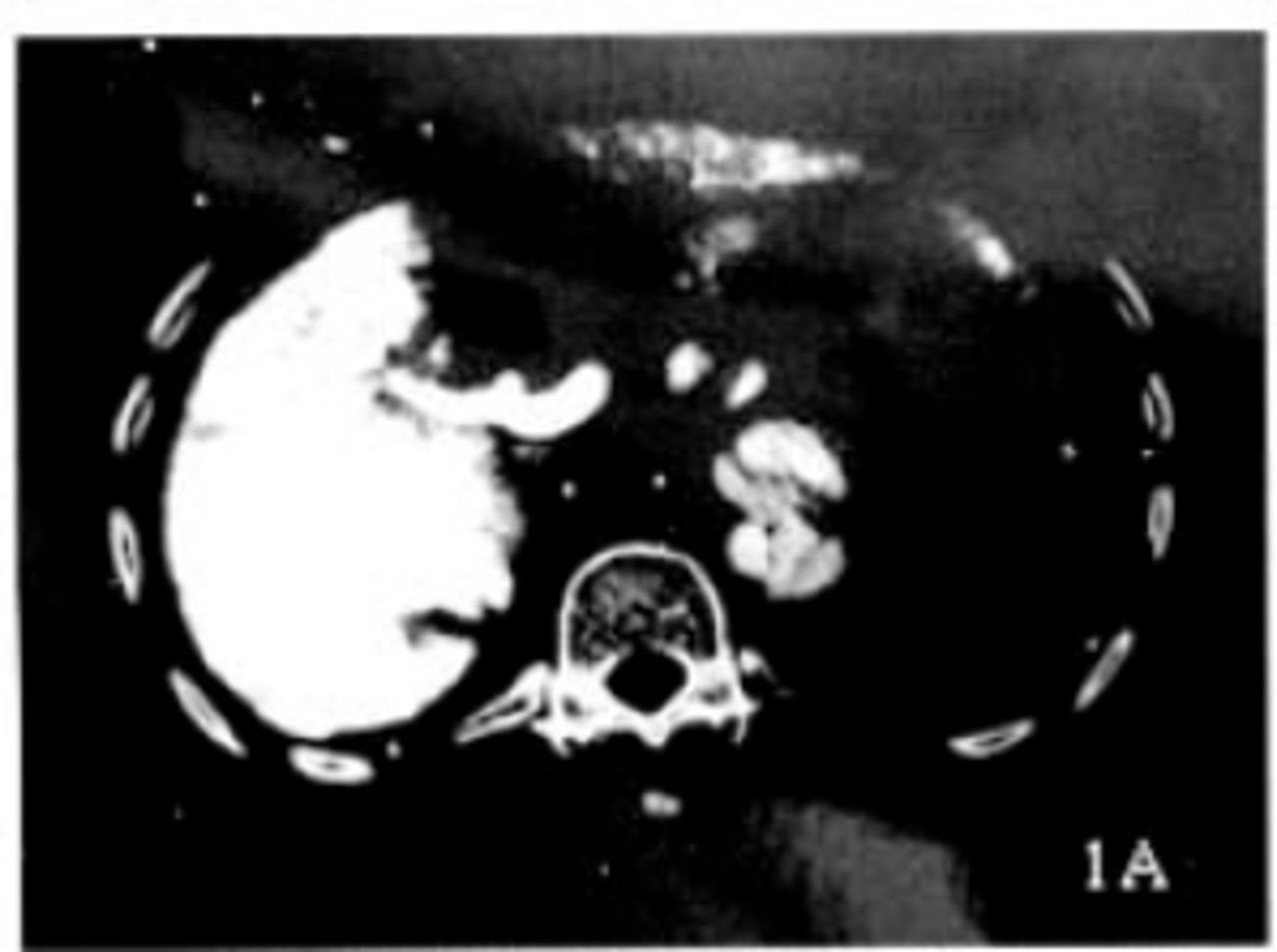
Erose or cuneate abnormal non-perfusion area appears in the right posterior lobe in CTAP 6-8 s after contrast agent is injected.
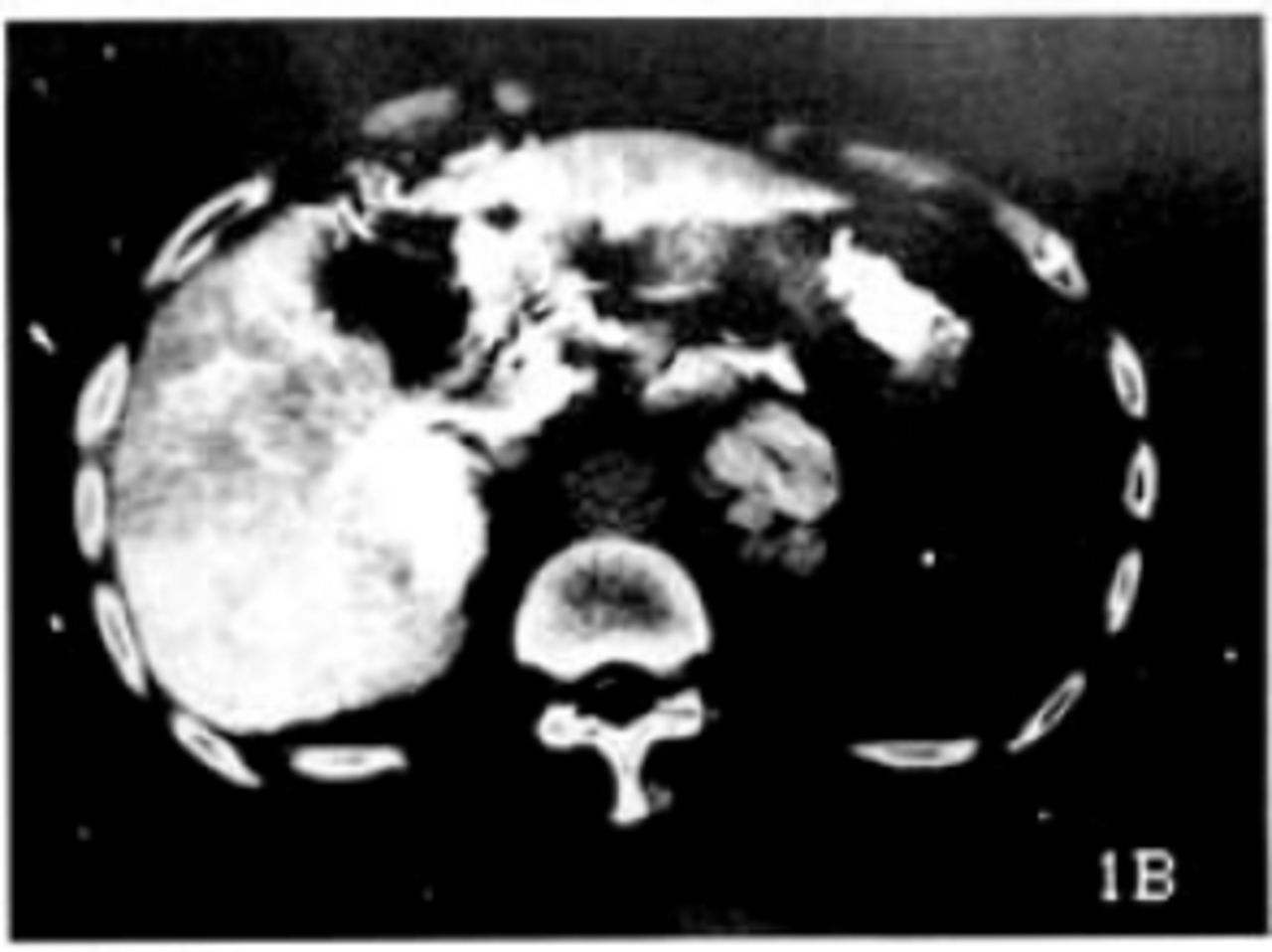
No enhancement can be seen in CTA, no pathologic changes are deleted.
DISCUSSION
With the development of helical CT, CTA and CTAP have been widely used in the diagnosis and differential diagnosis of hepatic tumors. The images of CTA and CTAP are much better than that of a regular CT scan, which helps to improve the sensitivity and specialty.[1-3]
CTA and CTAP seem to be useful to diagnose focal lesions within the liver. At the present time, the standard technique is as follows: a sequence-scan of the whole liver should be performed at 3~8 s after injection during CTA, but at 25~35 s after injection during CTAP. However, with the extensive use of CTA and CTAP, the frequency of non-cancerous abnormal perfusion in CTAP and non-pathological enhancement in CTA will become higher. In this series, the frequency of non-pathological enhancement was 14.2%, and the frequency of non-cancerous abnormal perfusion in CTAP was 19.9%. [4] The reason could be many variant factors which may affect the scan in the liver parenchyma such as hepatocirrhosis, local fatty degeneration, drainage veins under the capsule, post-operative changes of blood flow and the disturbance of lipiotol post interventional treatment. Other authors have reported the frequency of non-pathological enhancement can reach 33.3% 6~8 s after injection.[1,5,6] Since many factors such as those mentioned above may affect the results of CTA and CTAP, it is important to find a proper time to sequence-scan.[7]
There have been no reports concerning how to avoid the effect of depletion of the contrast medium and to reduce the frequency of abnormal perfusion within the liver at the same time. In this study, it was shown that sequence scaning of a proper time after contrast medium injection can improve an accurate diagnosis. There were unambiguous diagnoses in all 21 patients by the CTA and CTAP scan. There were three patients who received TACE by lipoidol sedimentation in the primary focus which resulted in abnormal perfusion within the liver at 6~8 s after injection during CAT, and thus prevented finding the lesions. [8] The contrast between lesions and normal liver tissue was decreased after 60 s and thus the lesions were difficult to detect. We have concluded from this study that the sequence scans of the whole liver 6~30 s after contrast agent injection in CTA and 30-60 s after in CTAP can improve detection of the lesions (Fig. 1).
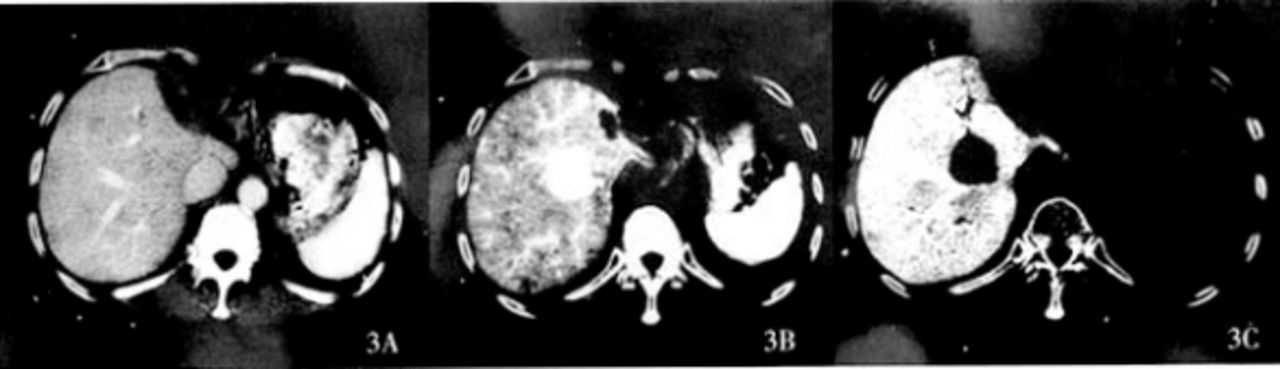
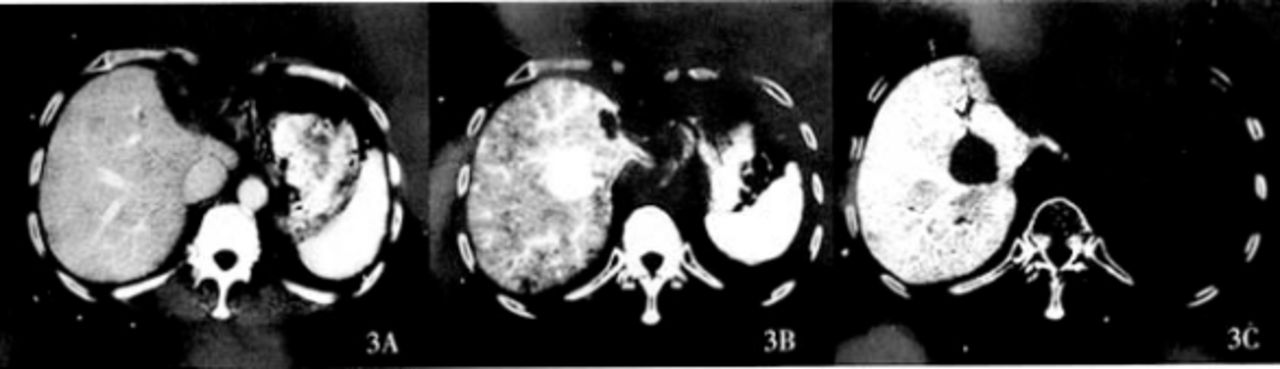
We should not evaluate the lesions only by the characteristics of CTA or CTAP, for the separate non-perfusion area in CATP or non-pathological enhancement in CTA may cause errors in diagnosis. When focus in the liver showed non-perfusion in CATP but enhanced in CTA, the diagnosis of hepatocellular carcinoma could be more certain. Our results suggest that a dynamic scan within the optional scan time can greatly reduce false-positive result by excluding the exceptional perfusion and the non-pathological enhancement. Thus, CTA and CATP are more effective techniques to detect hepatocellular carcinoma, to define the position of the lesions and to estimate the feasibility of resection (Figs.2,3).

Much of non-pathological enhancement appears in CTA 6 s after contrast agent is injected.
The focus in the right posterior lobe is clearly shown 30 s after contrast agent is injected.
The density of the focus in the right posterior lobe is equal to the normal liver tissue 30 s after contrast agent is injected, the focus in right anterior lobe is the sediment of lipiotol.
The focus cannot be seen clearly in a normal CT scan.
The focus can be clearly seen 8 s after contrast agent injection in CTA in a post-operation patient.
A further revealing of the focus can be seen in CTAP 30 s after contrast agent is injected.
- Received November 14, 2004.
- Accepted April 13, 2005.
- Copyright © 2005 by Tianjin Medical University Cancer Institute & Hospital and Springer
In this issue






{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.