

Abstract
OBJECTIVE To evaluate how arterial infusion chemotherapy after radical surgery influences long-term survival of patients with pathologic T3 (pT3) esophageal squamous carcinoma.
METHODS We divided 190 patients with pathologic pT3 esophageal squamous carcinoma, confirmed by consecutive radical surgery, into an experimental group (surgery + intra-arterial Infusion, 56 T3N0M0 and 52 TMMo cases), and the remaining patients into a control group (surgery alone, 48 T3N0M0 and 34 T3N,1M0 cases). The experimental group was sub-grouped into 56 cases (26 T3N0M0 and 30 T3N1M0 cases) receiving 1 or 2 periods of chemotherapy, while 52 cases (30 T3N0M0 and 22 T3N1M0 cases) underwent 3 or more than 3 periods of chemotherapy. We used one to seven courses of selected arterial Infusion chemotherapy of cisplatln (80 mg/m2 of body-surface area) and fiuorouracil (800 mg/m2) with or without epirubicin at 3~4 weeks post operation. The interval between each period was 3~4 weeks. All cases were followed-up for more than 5 years. Survival rates were calculated by the Kaplan-Meier methods and survival differences between patients with and without selected arterial Infusion chemotherapy were compared with the Log-rank test. Prognostic variables were entered Into a Cox regression analysis model controlling for age, site, lymph node status, and treatment received.
RESULTS The overall survival rates were not significantly different between the experimental group and the control group, but there was better survival for patients who received 3 or more than 3 courses of chemotherapy. Lymph node status (N) was an important factor in the prognosis.
CONCLUSION Transcatheter arterial Infusion chemotherapy is a safe and effective method of therapy. Postoperative selective arterial Infusion chemotherapy can improve the survival rate in patients with esophageal squamous carcinoma who were previously treated by radical surgery. However, this modality of therapy needs further investigation.
keywords
Multi-sample and multi-center studies have provided no evidence to indicate that preoperative chemo-radiation therapy can increase the 5 year survival rate of patients with esophageal squamous carcinoma, although some clinical studies have indicated that preoperative chemotherapy is effective. It is known that adjuvant chemotherapy after an operation can decrease the micro-metastases, but there have been few investigations as to whether it can increase the longterm survival rate, especially by use of arterial infusion chemotherapy. This research was designed to evaluate if arterial infusion chemotherapy influences long-term survival in pT3 esophageal squamous carcinoma patients after radical surgery.
MATERIALS AND METHODS
This study involved 190 patients with pT3 esophageal squamous carcinoma, from January 1990 to January 1999, who were treated with radical surgery. Their ages were 40-81 with a mean of 63 years, and were comprised of 158 males and 32 females. Their Karnofsky scores were over 70~80.
We adopted the AJCC-UICC 1997 stage classification to divide patients into an experimental group (108 cases, including 56 T3N0M0 and 52 T3N1M0 cases) and a control group (82 cases, including 48 T3N0M0 and 34 T3N1M0 cases). In addition the patients were further divided into 2 groups based on the number of chemotherapy treatments received. One group of 56 cases was treated lor 2 times (26 T3N0M0 and 30 T3N1Mo cases) and a second group of 52 cases received 3 or more treatments (30 T3N0M0 and 22 T3N1M0 cases). The Seldinger technique was used to insert a catheter into the celiac trunk artery. Routine DSA was employed, using compound meglumine diatrizoate. The 40%~50% of a dose of 10 ml and flow velocity of 5 ml/s (cisplatin 40 mg and fluorouracil 1 g) was diluted into 40-50 ml of saline and injected intra-arterially over 15 min. The catheter was immediately removed after administration of the drugs, the puncture was pressed for 15~20 min, and bandaged with pressure for 12~24 h. Limb movement was restricted for 6~8 h, and like with venous chemotherapy, the patients were monitored for back pain, and limb numbness. Routine blood tests and kidney and hepatic function were assessed 1 week after operations, and again every 4~6 weeks. After 2~3 determinations the efficacy of the therapy was evaluated. Statistics: SPSS 10.0 software was utilized, and the Kaplan-Meier survival analysis (Log-rank test), and the COX proportion risk model used to evaluate the important factors effecting prognosis.
RESULTS
Because there is no specific marker to determine the effectiveness of radical treatment of esophageal squa-mous carcinoma, only long-term follow-up of the survival rate can be used to determine the efficacy of the arterial infusion chemotherapy. As to our study, there was no statistically significant difference between the mean survival time of the two groups (Table 1). The results were the same even when the cases were divided into the presence or absence of lymphatic metastasis (Table 2,3).
Survival analysis between the experimental and control groups
Survival analysis of T3N1M0 cases between the experimental and control groups
Survival analysis of T3N0M0 cases between the experimental and control groups
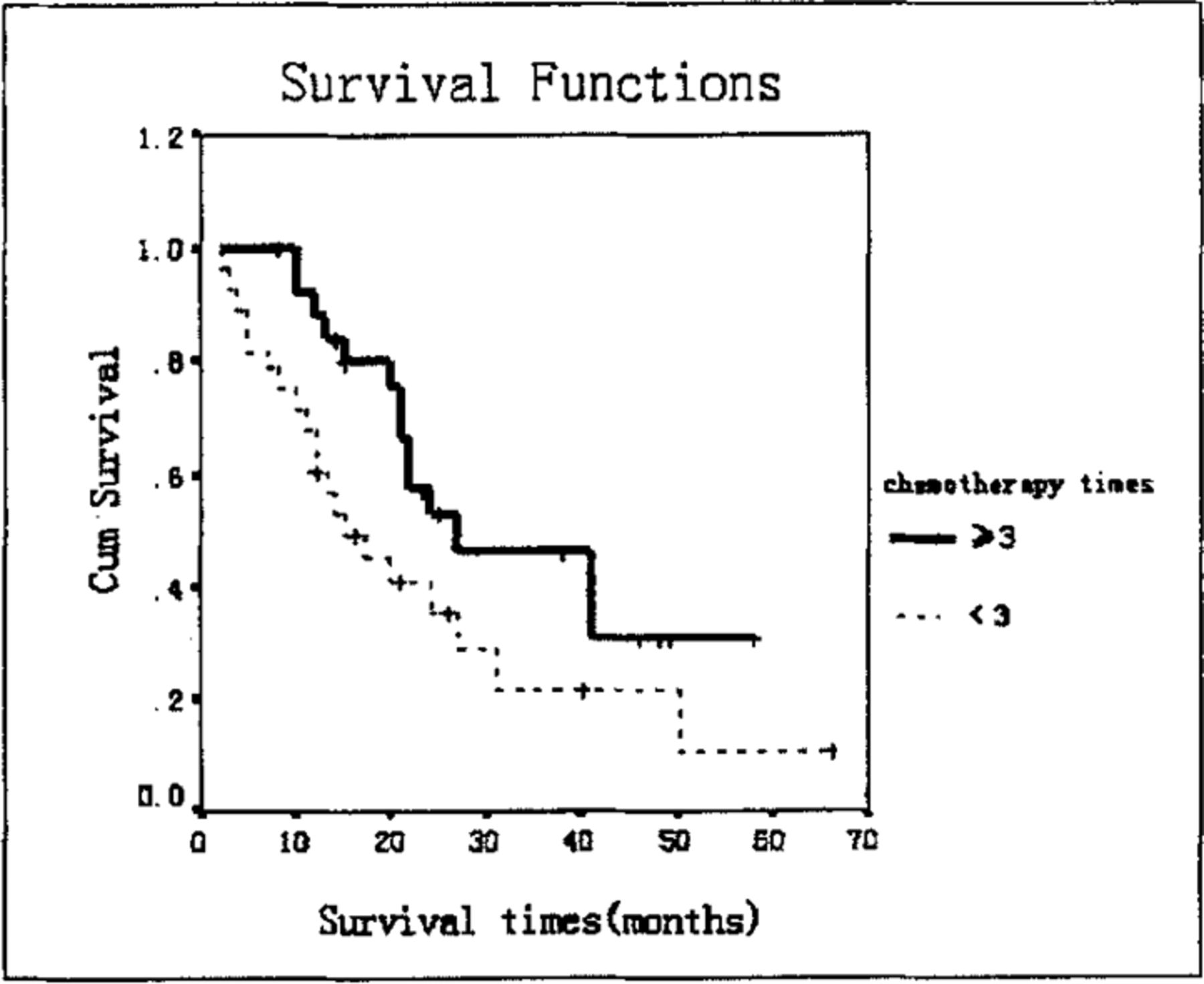
Comparison of survival times between patients receiving chemotherapy 3 times or more than 3 courses versus those treated less than 3 times showed a significant difference (Table 4, Fig.1). When the same analysis was conducted discounting lymphatic metastasis, the results showed that the number of chemotherapy treatments did not effect the long-term survival rate (Table 5, 6).
The mean survival time based on the chemotherapy times of treatment
The mean times in T3N0M0 survival time for the chemotherapy
The mean survival time based on the chemotherapy times of treatment in T3N1M0 cases
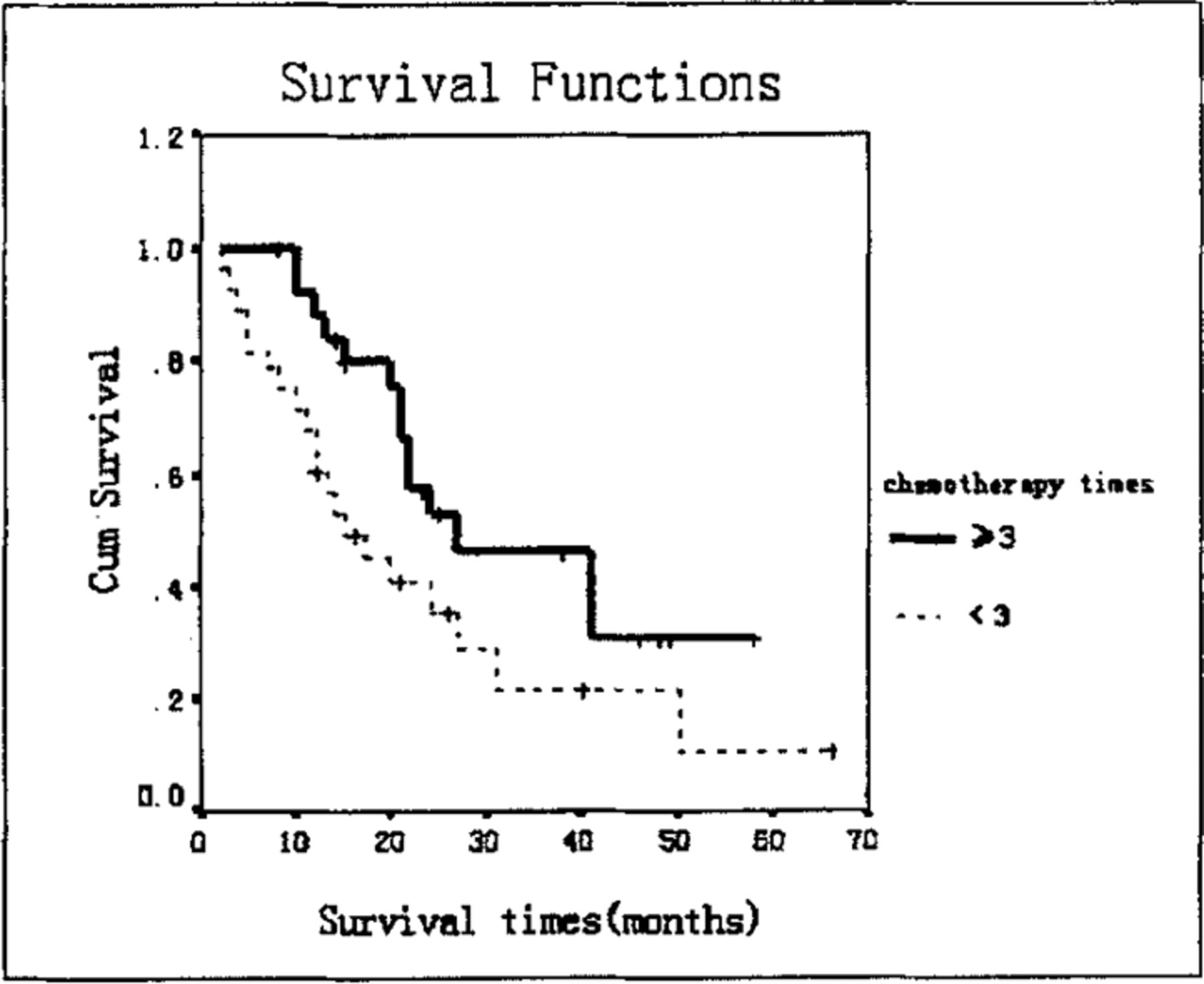
Long-term survival was influences by the number of chemotherapy treatments in pT3 esophageal squamous carcinoma patients after radical surgery.
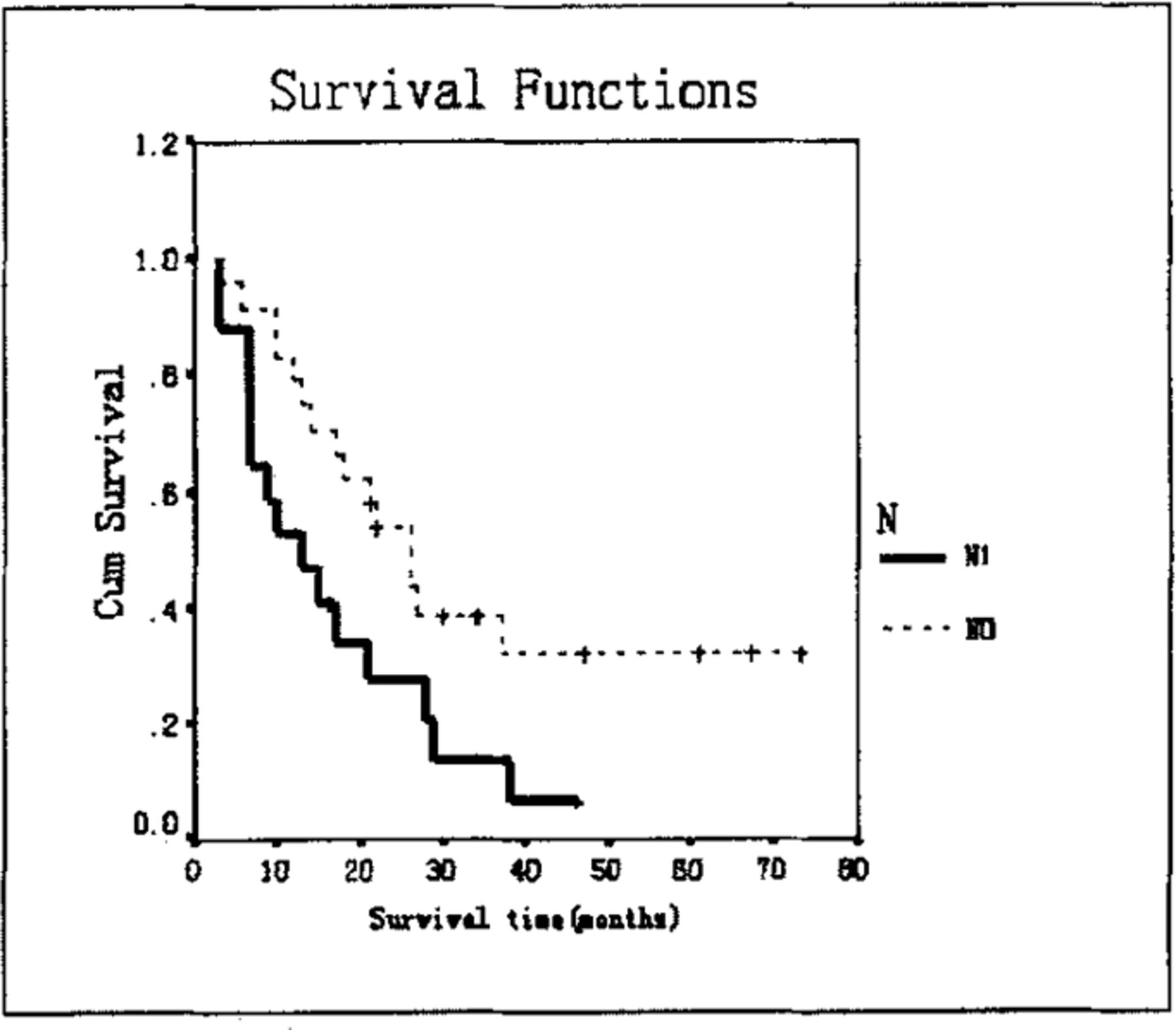
Cox proportion risk model analysis, Wald = 8.510, p = 0.004, showed that N is the key factor effecting the prognosis of esophageal squamous carcinoma (Table 7, Fig.2).
Mean survival time based on the N in esophageal squamous carcinoma

Long-term survival was influenced by lymph node status (N) in pT3 esophageal squamous carcinoma patients after radical surgery.
Side effects: no severe complications occurred but only low fever, nausea and upper abdominal discomfort. No treatment was needed and all the symptoms disappeared after 2-3 days.
DISCUSSION
Esophageal squamous carcinoma is still a common tumor in China, although its mortality and incidence rates recently have decreased.[1] The pathologic classification in Asia is mainly squamous carcinoma, while in Western countries, adenocarcinoma has greatly increased accounting for 40~50% of the cases.[2-4] Excision has long been recommended as the best mode of treatment.
It is estimated that 70%~80% of the patients have no chance of having an operation. Because of the special anatomical location of the esophagus, it is difficult to detect the tumor early except in areas where there is a high incidence. Although operation techniques have improved greatly, the long-term survival rate needs to be improved.
The five-year survival rate for patients with esophageal squamous carcinoma is lower than 10% at present, and even for those cases which are considered to be curable, the five-year survival rate is only around 20%~30%. Squamous carcinoma should be considered to be a systemic disease, whether or not there are early lymphatic métastasés. Furthermore, it is a multicenter disease, and early squamous carcinoma has unlocalized pathological changes, so the general treatment is useful for the middle and late stages of esophageal squamous carcinoma.
The usual treatment of a combined operation and systemic chemotherapy, often produces unsatisfactory results for the following reasons. Patients suffer from chemotherapeutic side effects, the tumor may have poor circulation so the drug level can not reach a therapeutic concentration, and only a portion of the cancer cells are in a proliferative stage. Some investigations have shown that neajuvant chemotherapy can increase the excision rate, but studies of the total survival rate with multi-centers, and a large cohort are needed.[5-8]
The effect of chemotherapy is not only related to the sensitivity of the tumor to the pharmacological action of the drug, but also proportional to the drug concentration and the time it is in contact with the tumor.[9-11] Accordingly, selective arterial infusion chemotherapy can increase the efficacy of treatment, and lessen the side effects caused with venous chemotherapy by increasing the drug concentration at the target organ, and by lengthening the contact time with the drugs. Thus in the early 1950’s, Klopp tried to inject anti-tumor drugs through the arteries that supply blood for the tumor. Up to now hepatic arterial infusion chemotherapy for treating liver cancer has been widely used. In 1975, Tanohata first used angiography combined with arterial infusion chemotherapy to treat esophageal squamous carcinoma. Intravascular intervention has now become a new branch of clinical medicine.
Indications for esophageal squamous carcinoma arterial infusion chemotherapy are now unclear but may include the following: 1) if there are no métastasés, localized in the artery supplying the esophageal segment. 2) for thorax esophageal squamous carcinoma which has invaded the surrounding organs, operation after chemotherapy is recommended. 3) if the tumor has vascular supply which is confirmed by angiography.
Contraindications include main organ dysfunction, valetudinarianism, coagulation dysfunctions, infection, fever, perforation and bleeding.
Complications include thrombosis, haematoma, infection, esophageal ulcer bleeding and so on. Among the complications, spinal cord injury is the most serious. The reasons may be: 1) the toxicity of ion-type contrast agents. 2) 90% of the blood supply to the spinal cord comes via the intercostal arteries (segmental arteries) which have few anastomoses, therefore, the left 5th intercostal arteries spasm resulting in spinal cord injury due to lack of a blood supply. 3) the catheter may obstruct the blood supply or cause vascular thrombosis. 4) the toxicity of the anti-tumor drugs.
Lower limb movements and sensations and so on should be observed in order to prevent spinal injury. It is quite important to be familiar with the anatomy of the blood supply for the target area as complex anastomoses and variance of the vascular supply makes arterial infusion chemotherapy difficult.
Studies of arterial infusion chemotherapy in China have indicated that the short-term effective rate is around 50%, suggesting that this procedure is mainly for late stage patients who are beyond receiving an operation. Our study showed that there was no significant difference between arterial infusion chemotherapy at pT3 postoperation compared to those in the late pT3 esophageal squamous carcinoma, but it can prolong the survival time.
COX proportion risk model analysis (Wald=8.510, P=0.004), showed that N was the key factor influencing prognosis. Our study indicated that the long-term survival rate was improved when 3 or more than 3 courses of arterial infusion chemotherapy were administered compared to fewer treatments.
Arterial-perfusion chemotherapy does not have a superiority over systemic chemotherapy treatment of tumors, which may be related to with the fact that the chemotherapeutics are unable to enter the tumor bed because of intraoperative ligation of the artery supplying the tumor tissue, and the level of drugs cannot be increased by collateral circulation. At present it is not clear if there is a benefit with postoperative arterial-perfusion chemotherapy, however, local recurrence or liver metastasis in this study was much less compared to the controls)[12]
A multi-center study with a large number of patients is needed, including the choice and combination of drugs. With the development of new drugs (paclitaxel, CPT11, Gemzar), production of new chemotherapeutic regimens, and molecular target treatment (Iressa),[13,14] the efficacy of arterial infusion chemotherapy can be improved in the future.
- Received January 12, 2006.
- Accepted May 22, 2006.
- Copyright © 2006 by Tianjin Medical University Cancer Institute & Hospital and Springer
In this issue






{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.