
Abstract
Objective: A meta-analysis was performed to augment the insufficient data on the impact of mutative EGFR downstream phosphatidylinositol-3-kinase (PI3K) and mitogen-activated protein kinase (MAPK) pathways on the clinical efficiency of epidermal growth factor receptor tyrosine kinase inhibitor (EGFR-TKI) treatment of non-small cell lung cancer (NSCLC) patients.
Methods: Network databases were explored in April, 2015. Papers that investigated the clinical outcomes of NSCLC patients treated with EGFR-TKIs according to the status of K-ras and/or PIK3CA gene mutation were included. A quantitative meta-analysis was conducted using standard statistical methods. Odds ratios (ORs) for objective response rate (ORR) and hazard ratios (HRs) for progression-free survival (PFS) and overall survival (OS) were calculated.
Results: Mutation in K-ras significantly predicted poor ORR [OR =0.22; 95% confidence interval (CI), 0.13-0.35], shorter PFS (HR =1.56; 95% CI, 1.27-1.92), and shorter OS (HR =1.59; 95% CI, 1.33-1.91) in NSCLC patients treated with EGFR-TKIs. Mutant PIK3CA significantly predicted shorter OS (HR =1.83; 95% CI, 1.05-3.20), showed poor ORR (OR =0.70; 95% CI, 0.22-2.18), and shorter PFS (HR =1.79; 95% CI, 0.91-3.53) in NSCLC patients treated with EGFR-TKIs.
Conclusion: K-ras mutation adversely affected the clinical response and survival of NSCLC patients treated with EGFR-TKIs. PIK3CA mutation showed similar trends. In addition to EGFR, adding K-ras and PIK3CA as routine gene biomarkers in clinical genetic analysis is valuable to optimize the effectiveness of EGFR-TKI regimens and identify optimal patients who will benefit from EGFR-TKI treatment.
- Non-small cell lung cancer (NSCLC)
- tyrosine kinase inhibitor (TKI)
- targeted therapy
- K-ras
- PIK3CA
- meta-analysis
Introduction
Lung cancer remains the leading cause of cancer death in both genders according to the most recent statistics of the American Cancer Society1. Non-small cell lung cancer (NSCLC) accounts for more than 85% of lung cancers2. Most patients present with advanced NSCLC at the time of diagnosis, and chemotherapy becomes their palliative option. However, the poor improvement in the clinical response and survival outcomes of NSCLC patients who underwent chemotherapy over the last two decades highlights the need for more effective and less toxic treatments3.
Epidermal growth factor receptor tyrosine kinase inhibitor (EGFR-TKI) is a small-molecule drug that targets the active adenosine triphosphate binding site of EGFR kinase. Recent studies on patients bearing sensitive EGFR mutation have shown that EGFR-TKIs effectively increase clinical response rate and improve patients’ survival compared with standard chemotherapy, such as cisplatin plus gemcitabine or carboplatin plus paclitaxel, by inhibiting autophosphorylation and activation of downstream signaling pathways4–7. NSCLC patients harboring EGFR mutations benefit more from EGFR-TKI treatment than those without EGFR mutations. However, several studies demonstrated that gene mutations on the EGFR downstream signal pathways are also significant for the response of NSCLC patients to EGFR-TKIs.
EGFR activation elicits its effects via the K-ras/BRAF/mitogen-activated protein kinase (MAPK) and phosphatidylinositol-3-kinase (PI3K)/AKT/mTOR pathways, which promote tumor proliferation, invasion, migration, and neovascularization8. Mutation in the downstream genes of EGFR signaling pathways may result in receptor-independent pathway activation that renders the tumors unresponsive to EGFR inhibition. K-ras and PI3K are the key regulators on the two aforementioned pathways, respectively. K-ras encodes RAS, a guanosine triphosphate (GTP)-binding protein, which phosphorylates and activates MAPK by interacting with downstream BRAF, leading to a cascade of kinase reactions9. K-ras mutation attenuates the intrinsic GTPase activity of RAS protein, resulting in prolonged RAS activation10. The PIK3CA gene encodes the p110α catalytic subunit of PI3K protein, and its mutation leads to constitutive activation of protein kinase B signaling11. Both pathways play an important role in various cell physiological and pathological processes, such as proliferation, differentiation, apoptosis, and cell migration12–14. Although the corresponding frequencies of K-ras and PIK3CA mutations are approximately 5%-15% and 3%-5%15,16, many studies have reported that K-ras and PIK3CA mutations may have primarily induced resistance to EGFR-TKIs of NSCLC patients17,18.
A previous meta-analysis19 indicated a significant correlation between K-ras mutation and clinical response of NSCLC patients treated with EGFR-TKIs. However, the study merely focused on the objective response rate (ORR), and valuable information on the impact of K-ras mutation on the survival of NSCLC patients treated with EGFR-TKIs was not provided because of insufficient data. Similar studies on PIK3CA mutation are rarely reported. Thus, limited information on the clinical significance of gene mutations in the EGFR downstream signal pathways, especially for K-ras and PIK3CA, in NSCLC patients treated with EGFR-TKIs is available.
Therefore, we performed a meta-analysis of published studies to assess the impact of K-ras and PIK3CA mutation on the ORR, progression-free survival (PFS), and overall survival (OS) of NSCLC patients treated with EGFR-TKIs to clarify whether these mutations attenuate the clinical benefits of EGFR-TKI treatment in NSCLC patients.
Materials and methods
Search strategy
We developed a search strategy. An internet search of PubMed, EBSCO, OvidSP, and Wiley Online database was performed in April, 2015. Gefitinib and erlotinib, which are the first-generation EGFR-TKIs, had similar efficacies in NSCLC patients20,21. Thus, a combination of a disease domain (“lung cancer”), a treatment domain (“gefitinib”, “erlotinib”, or “EGFR TKI”), and a gene domain (“kras” or “pik3ca”) was used in all fields. The language was limited to English. All retrieved results were sent to EndNote software (EndNote X6, THOMSON REUTERS, US) to automatically and manually check for duplicate studies. After removing the duplicates, the titles and/or abstracts of the remaining results were screened to exclude irrelevant articles. Full texts of relevant articles were obtained and screened further for eligible studies. Bibliographies of relevant articles were hand-searched to determine additional eligible studies.
Selection criteria
Two reviewers carefully and independently investigated all studies identified, and consensus was reached after discussion when disagreement in the inclusion or exclusion of studies was encountered. Inclusion criteria were as follows: (I) studies focused on NSCLC patients; (II) studies explored the relation between mutations of K-ras or PIK3CA and outcomes of NSCLC patients treated with EGFR-TKIs; and (III) studies assessed anti-tumor response using one or more of the following parameters: ORR, PFS, and OS. Distinguishing the predominant effect of the EGFR-TKI treatment was difficult when patients underwent combined therapy treatment. Therefore, exclusion criteria were as follows: (I) patients were not treated with single EGFR-TKIs; and (II) PFS and OS were not calculated from the initiation of EGFR-TKI treatment. When the same patient population was used in several publications, only the most recent, complete, or largest study was included in the meta-analysis.
Data extraction
Data from all eligible studies were extracted independently by two researchers with disagreement settled by discussion. The following data from eligible studies were collected: publication details (such as the first author’s last name, publication year, and country in which the study was performed), trial information (such as inclusion criteria, number of patients assessed, therapy regimens, genes detected and detection methods, and type of end points used), patient characteristics (such as age, gender, stage, and histology), and outcome measures [such as hazard ratios (HRs) for PFS and OS and their 95% confidence intervals (CIs), log-rank test P values, and ORRs]. PFS and OS were defined as starting from the initial EGFR-TKI treatment. For PFS and OS, the HRs and their 95% CIs were estimated by methods proposed by Tierney et al.22 in the absence of published HRs or their 95% CIs. For ORRs, the reported number of objective response (complete response + partial response) and no response (progressive disease + stable disease) in each arm was collected. Quality was assessed independently by two investigators using the Newcastle-Ottawa scale (NOS) for non-randomized studies (available at http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp) with consensus on all items through discussion.
Statistical analysis
The relationship between gene mutation and ORR was presented by odds ratio (OR) with 95% CI. The impact of gene mutation on PFS and OS was measured by HR with 95% CI. The pooled ORs were computed for dichotomous variables by the Mantel-Haenszel method, and the pooled HRs and their 95% CIs were estimated by a general variance-based method. Heterogeneity across studies was tested by the χ2-based Q-test and I2 statistic. A P value greater than 0.10 for the Q-test and I2 statistic with values no more than 50% indicate the lack of heterogeneity among studies. Thus, the fixed-effect model was used for meta-analysis; otherwise, the random-effect model was used. Sensitivity analysis was conducted for meta-analyses by removing one study at a time to test the robustness of the overall results. Potential publication bias was estimated using Begg’s funnel plots and Egger’s linear regression test. All statistical tests were performed with STATA 12.0 (STATA Corporation, College Station, TX). All reported P values were two-sided. Differences were considered statistically significant at P<0.05.
Results
Literature search and study characteristics
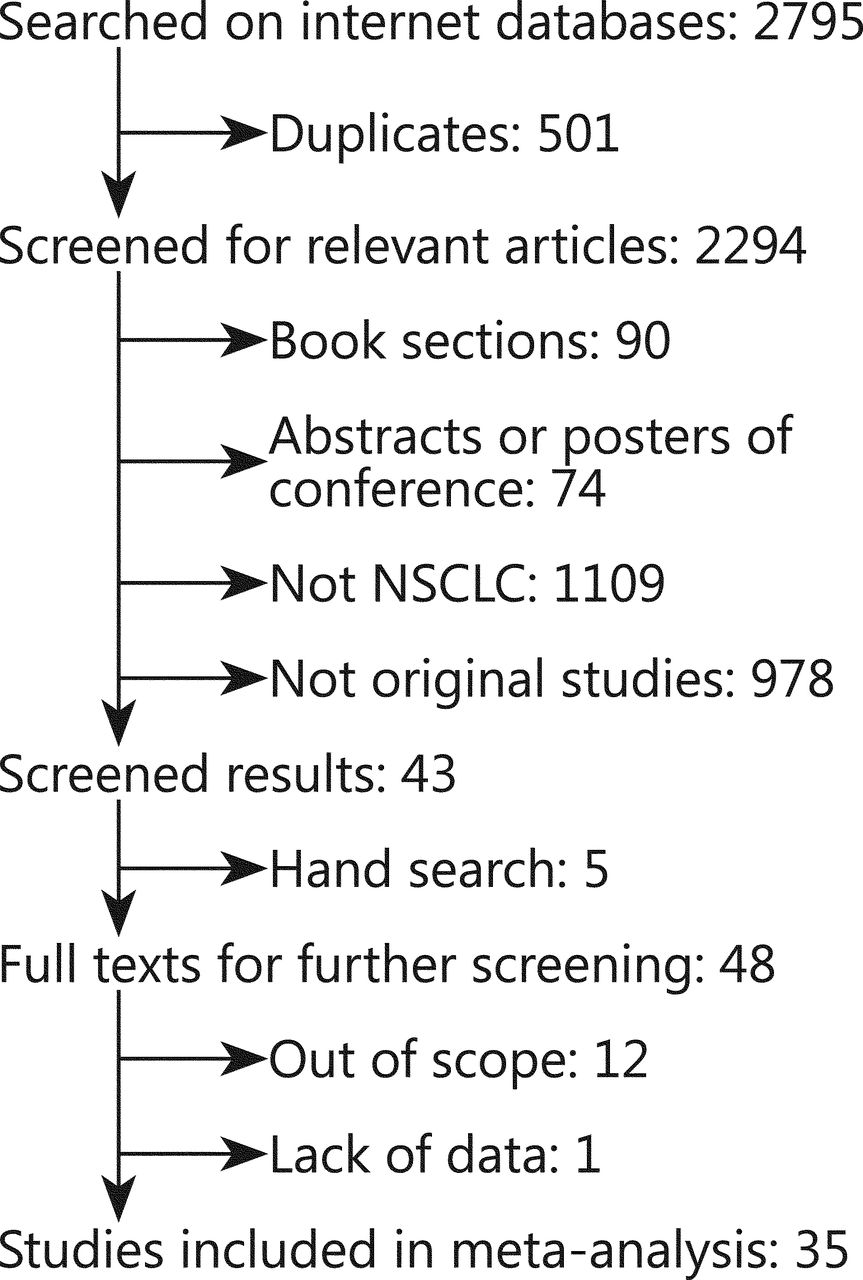
The initial search on PubMed, EBSCO, OvidSP, and Wiley Online database in April, 2015 retrieved 2,795 studies. A total of 2,294 articles remained after 501 duplicates were removed. After preliminary screening of titles and/or abstracts, 2,087 non-original or irrelevant studies, 90 book sections, and 74 abstracts or posters of conferences were excluded. Hand search on bibliographies of relevant articles retrieved five additional articles. Thus, full texts of 48 relevant studies were obtained for further investigation. Thirteen articles were further excluded because they were out of scope (12) and they lack relevant data (1). Finally, 19 articles23–41 published before 2010, 10 articles17,18,42–49 after 2010 and another 6 articles50–55 were included. The selection flow diagram is summarized in Figure 1.
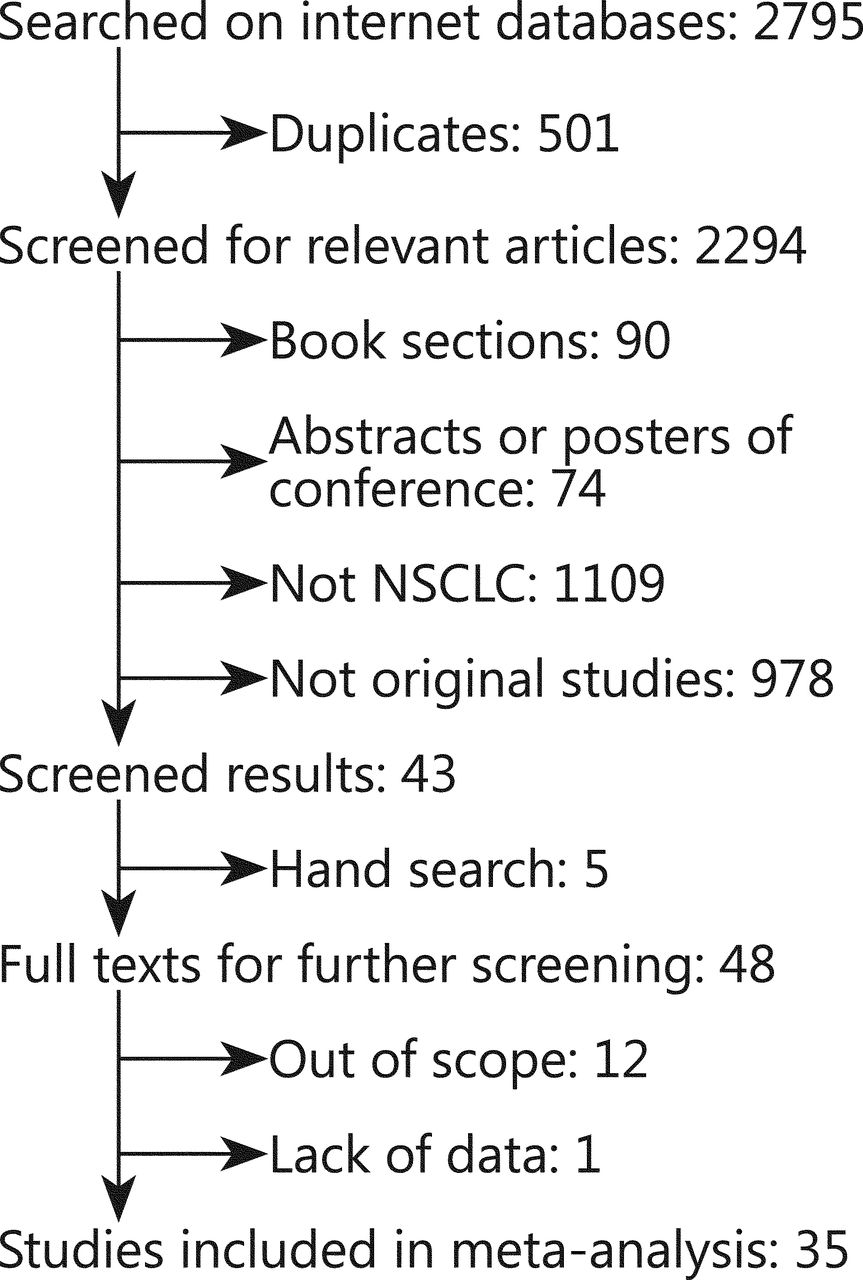
Flow diagram of selection process.
The 35 studies were published from 2006 to 2014. These studies were conducted worldwide: nine from Italy18,26,34–36,40,44,49,53, five from multi-centers (more than two countries or regions)33,39,42,51,52, five from the United States28,30,38,50,54, two from Netherlands29,48, three from Japan23,27,37, two from Korea17,25, two from Germany31,55, and the rest were from Switzerland24, Greece45, France43, Czech Republic47, China41, Mexico46, and Taiwan32. The median age reported in 28 studies ranged from 58 to 75. A total of 3,958 patients were included with a mean sample size of 113 (ranged from 15 to 393). Most studies included patients with NSCLC, with only five studies focused on lung adenocarcinoma17,35,36,49,50, and one focused on lung squamous carcinoma47. Except in two studies17,32, all patients had inoperable stage IIIB or IV or recurrence. Previous treatments included chemotherapy, radiotherapy, surgery, or none. Current treatments of all included studies were monotherapy with EGFR-TKIs. In studies with treatment details, patients were treated with erlotinib or gefitinib according to international standard with one patient who received PF00299804, an irreversible TKI of EGFR, HER2, and HER4, in a study17. Clinical response was evaluated using RECIST criteria56 in 31 studies and WHO criteria57 in three studies, with one study not reported. Patients with complete or partial responses were classified as responders in all studies. ORR was the end point of 30 studies, PFS in seven studies, and OS in 11 studies. HR and corresponding 95% CI for PFS and OS were calculated from the primary data reported in the text of one study17, and estimated from the reported summary statistics with method recommended by Tierney in two studies44,47. The quality of all included studies was assessed with NOS. The quality scores of all studies were above 7, with mean score of 8.3.
Biomarker analysis
A total of 33 studies provided the technological details for detecting gene mutations, and 16 studies performed mutation screening using direct sequencing (DS). The rest of the articles included pyrosequencing (1), denaturing capillary electrophoresis (DCE) (3), performance of amplification refractory mutation system (2), polymerase chain reaction (PCR)-restriction fragment length polymorphism (2), mutant-enrich sequencing (ME) (2), and denaturing high-performance liquid chromatography (2). A combination of the aforementioned methods was used in five studies. Mutation in K-ras exons 1, 2, and/or 3 was assessed in 34 studies, and PIK3CA exons 9 and/or 20 in 5 studies. Mutation of EGFR exons 18-21 was detected in all studies.
A total of 573 out of 3,377 evaluable patients were K-ras-mutation positive (17.0%), and 18 out of 473 patients were PIK3CA-mutation positive (3.8%). A total of 16 studies reported that K-ras mutation was mutually exclusive with EGFR mutation, and five other studies reported that 10 out of 178 patients positive for K-ras mutation were concomitant with EGFR mutation. Three studies reported that 6 out of 11 patients positive for PIK3CA mutation were concomitant with EGFR mutation. Table 1 shows the main characteristics of studies included in the meta-analysis.
Main characteristics of studies included in the meta-analysis
Predictive value of K-ras mutation
The impact of K-ras mutation on the ORR of NSCLC patients treated with EGFR-TKI therapy was evaluated based on 29 studies (Table 2). K-ras mutation was associated with reduced objective response in NSCLC patients with a pooled OR of 0.22 (95% CI, 0.13-0.35) (Figure 2A). Fixed-effect model was used because heterogeneity across the trials was not significant (I2=0%; P=0.999). The sensitivity analysis indicated that no individual study changed the pooled OR significantly (Figure 2B), suggesting that the result was reliable. Publication bias was significant in Begg’s test (P=0.049), but not in Egger’s test (P=0.090) (Figure 2C). Patients included in two studies39,54 apparently originated from the same center. Given that the independence of the two studies could not be confirmed, another analysis excluding the prior one of the aforementioned studies was conducted considering the possibility of duplicate patient population. The pooled OR was 0.22 (95% CI, 0.13-0.35) in a fixed effect model (I2=0%; P=0.998), with publication bias reduced significantly (P values in Egger’s and Begg’s tests were 0.101 and 0.072, respectively).
Pooled results of meta-analysis of the predictive value of K-ras and PIK3CA mutation in patients with NSCLC
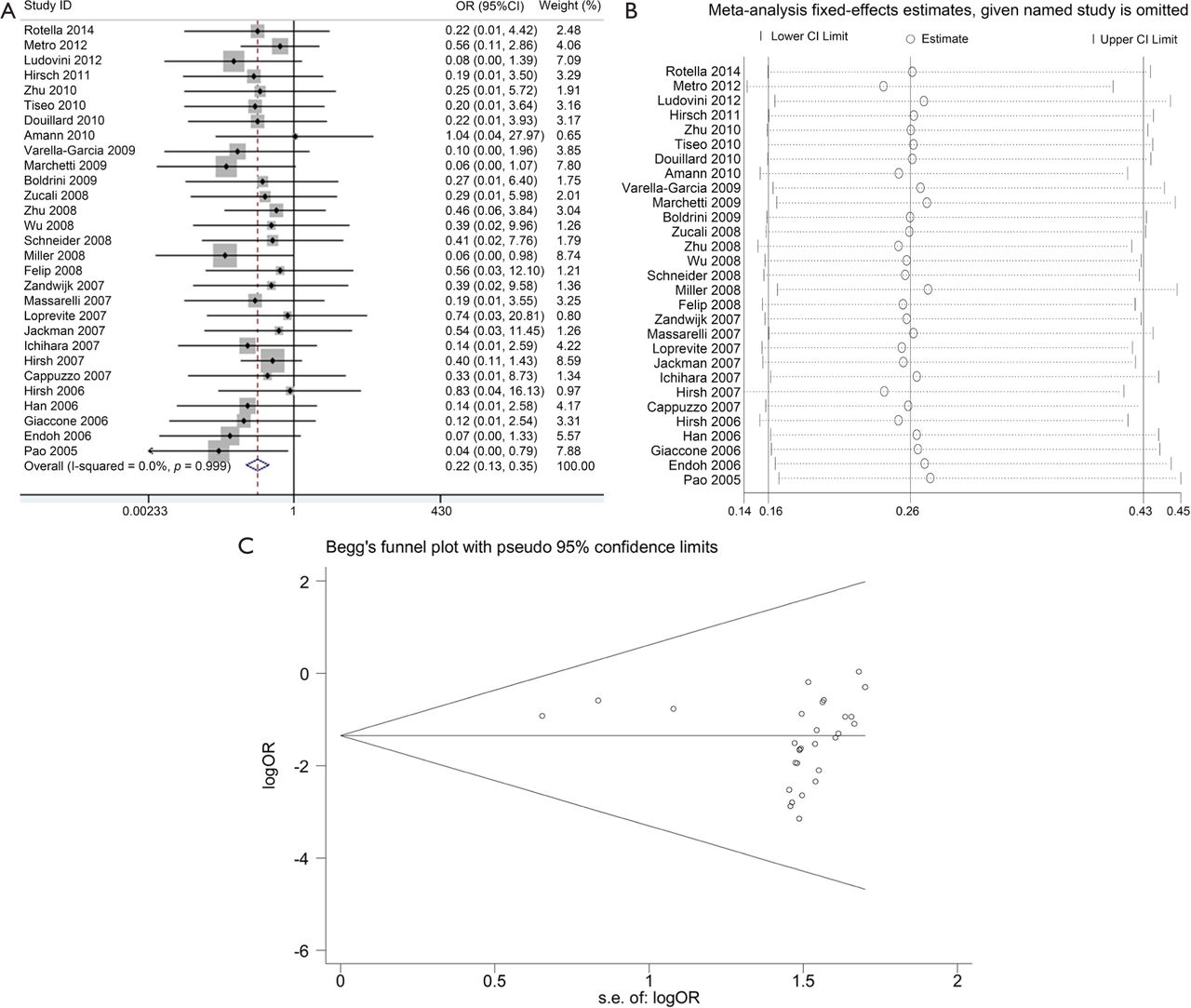
Meta-analysis of the predictive value of K-ras mutation for ORR. (A) Forest plots of OR and 95% CI; (B) Results of sensitivity analysis; and (C) Begg’s funnel plot analysis of publication bias. OR, odds ratio; ORR, objective response rate; s.e., standard error.
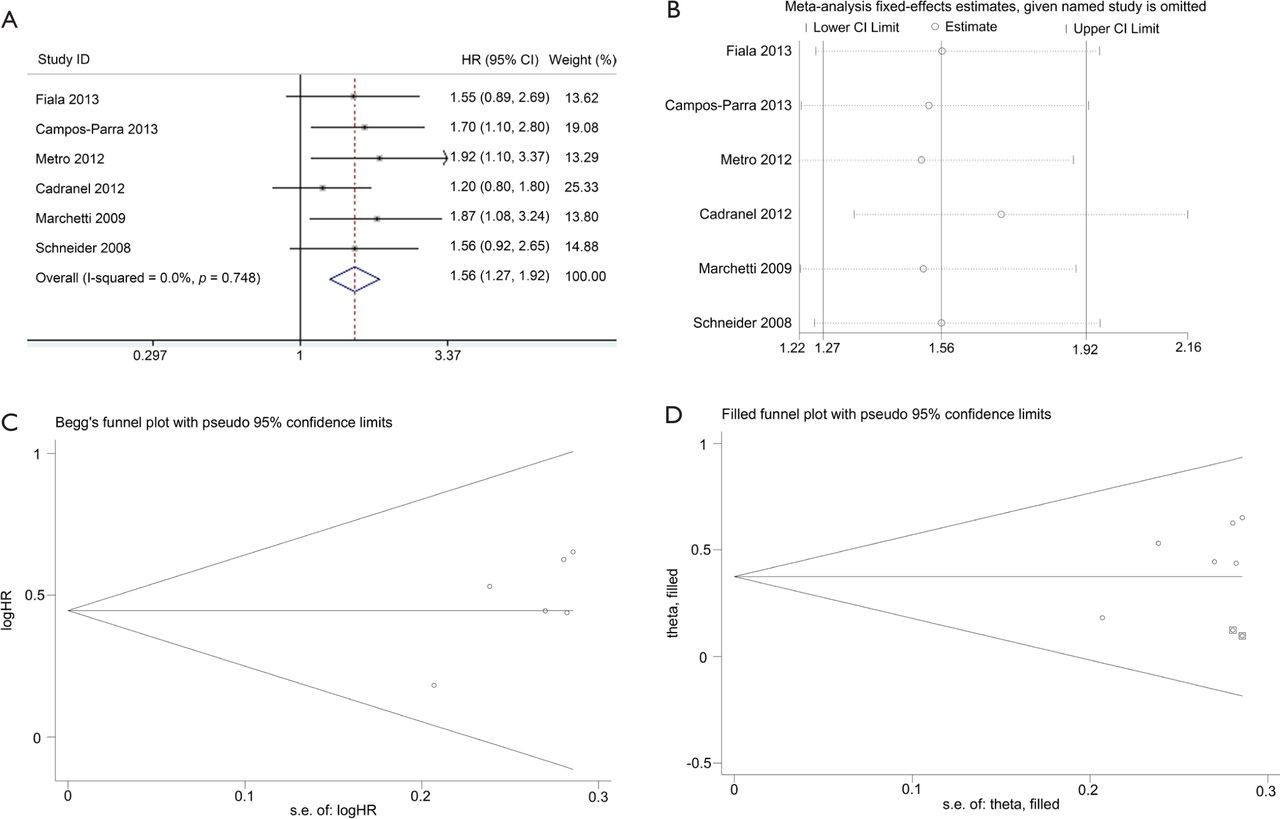
Data for assessing the impact on PFS according to K-ras mutation status was available in six studies. K-ras mutant patients had shorter PFS compared with wild-type patients with pooled HR of 1.56 (95% CI, 1.27-1.92) (Figure 3A). Fixed-effect model was used when calculating pooled HR for PFS because heterogeneity across trials was not significant (I2=0%; P=0.748). Sensitivity analysis indicated that this result was robust (Figure 3B). Egger’s test revealed slight publication bias (P=0.046), contrary to Begg’s test (P=0.260) (Figure 3C). Thus, a non-parametric “trim-and-fill” method was utilized to adjust the publication bias (Figure 3D). After the trim-and-fill adjustment, two missing studies were added, and the estimated pooled HR was 1.46, with 95% CI ranging from 1.21 to 1.74.
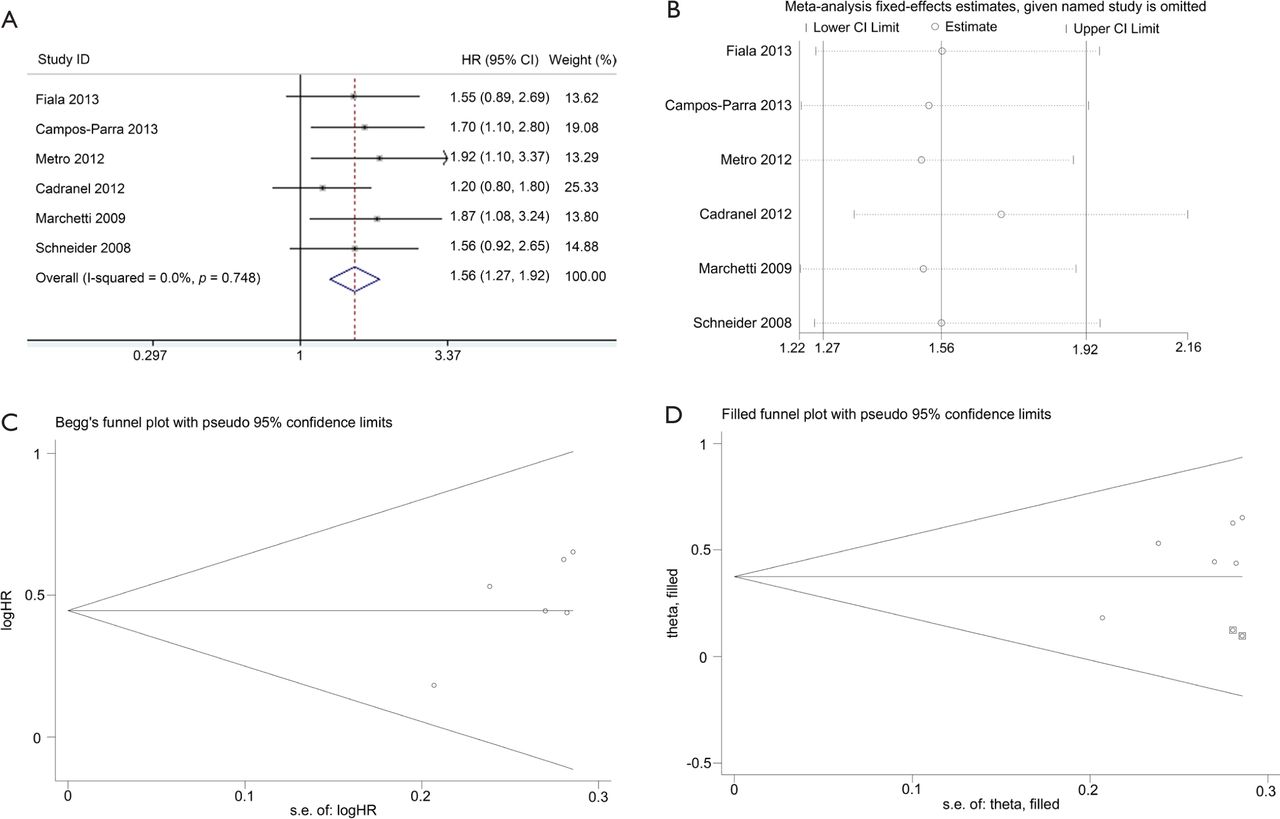
Meta-analysis of the predictive value of K-ras mutation for PFS. (A) Forest plots of HR and 95% CI; (B) Results of sensitivity analysis; (C) Begg’s funnel plot analysis of publication bias; and (D) Filled funnel plot using trim-and-fill method. ○, indicates observed studies; ◙, indicates missed studies. HR, hazard ratio; s.e., standard error.
Ten studies were available for analyzing the impact on OS according to K-ras mutation. Results showed that NSCLC patients with K-ras mutation had shorter OS than wild-type patients with pooled HR of 1.59 (95% CI, 1.33-1.91) (Figure 4A). A fixed-effect model was used in calculating pooled HR for OS because heterogeneity across the trials was not significant (I2=22.8%, P=0.233). Sensitivity analysis indicated that the result was stable (Figure 4B). Publication bias was not significant in both Egger’s (P=0.098) and Begg’s tests (P=0.210) (Figure 4C).
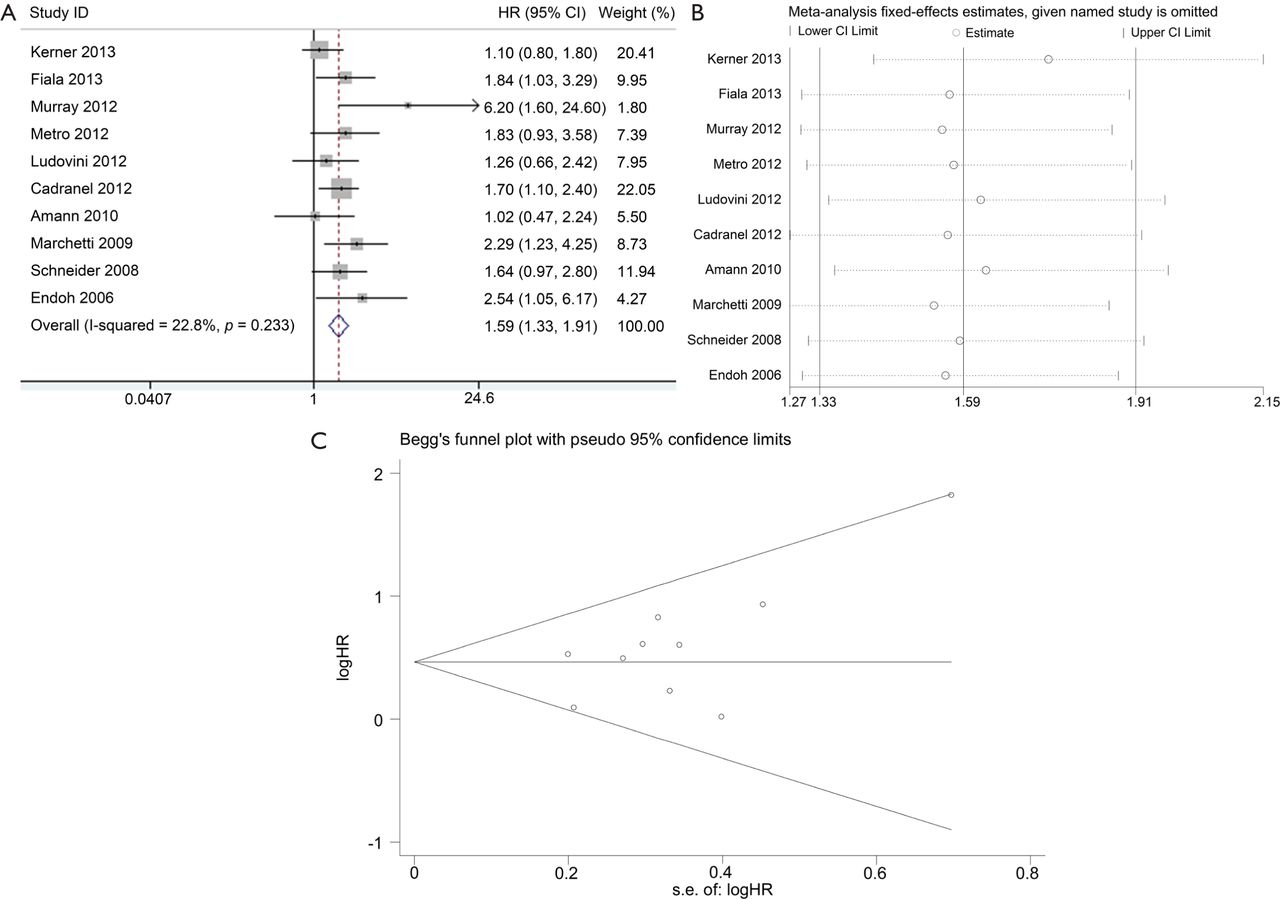
Meta-analysis of the predictive value of K-ras mutation for OS. (A) Forest plots of HR and 95% CI; (B) Results of sensitivity analysis; and (C) Begg’s funnel plot analysis of publication bias. HR, hazard ratio; s.e., standard error.
To determine the slight heterogeneity across trials in the analysis of the impact of K-ras mutation on the OS of NSCLC patients treated with EGFR-TKIs, we conducted subgroup analysis based on whether K-ras mutation is concomitant with EGFR mutation, previous treatment, and mutation detection method (Table 3). Heterogeneity across trials decreased in most subgroups (Table 3). In addition, a negative effect of K-ras mutation on the OS of NSCLC patients with EGFR-TKI treatment was observed in all subgroups, which further confirmed the robustness of the general result.
Predictive value of PIK3CA mutation
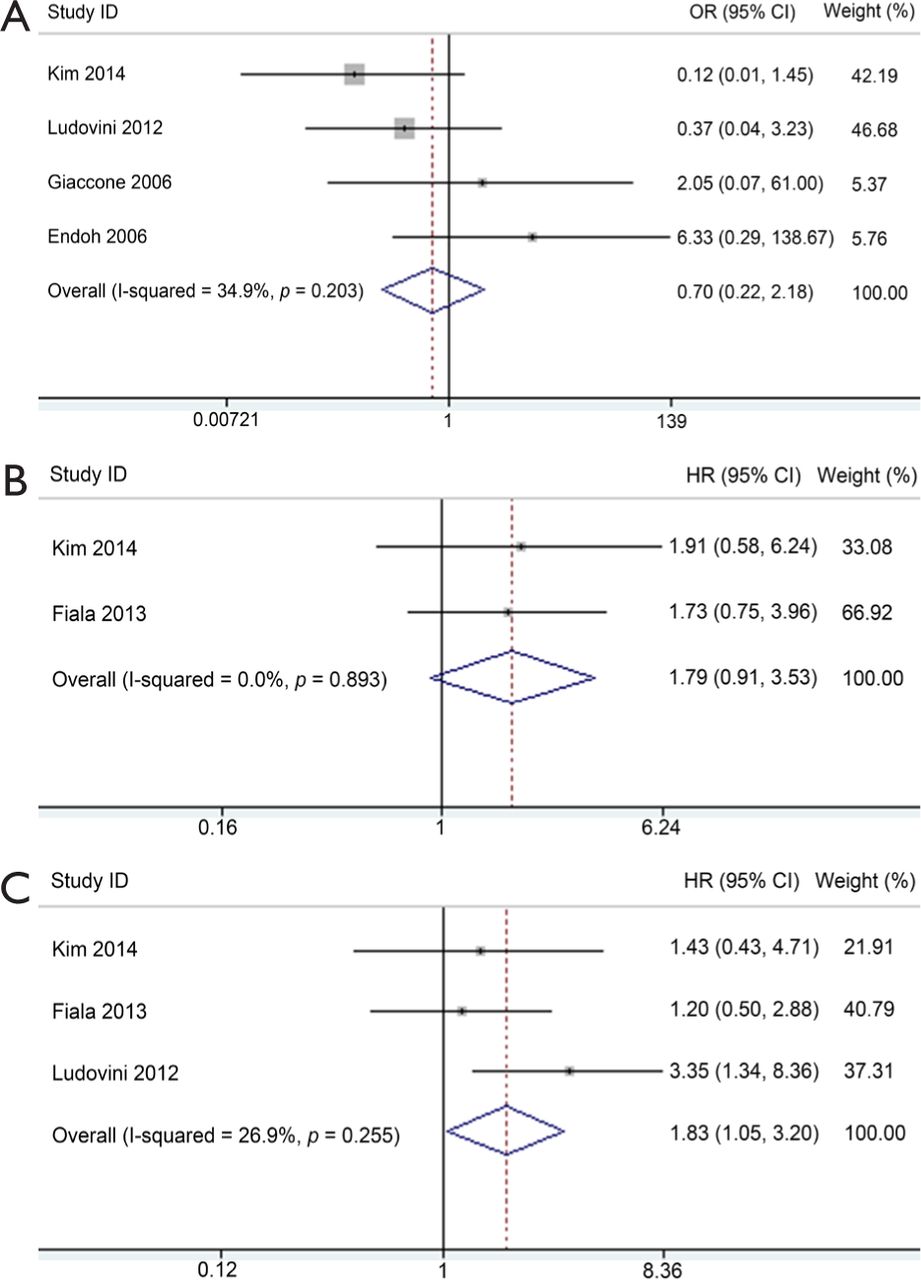
Five studies investigated the predictive role of PIK3CA mutation in NSCLC patients (Table 2). Among these, ORR data were available in four studies, PFS data in two studies, and OS data in three studies. PIK3CA mutant NSCLC patients exhibited similar response to EGFR-TKIs compared with wild-type patients with corresponding pooled OR of 0.70 (95% CI, 0.22-2.18) (Figure 5A). Fixed-effect model was used because heterogeneity across studies was not significant (I2=34.9%; P=0.203). The pooled HR of 1.79 (95% CI, 0.91-3.53) for PFS in a fixed-effect model (I2=0%; P=0.893) suggested that PIK3CA mutant NSCLC patients had similar PFS compared with wild-type patients when treated with EGFR-TKIs (Figure 5B). However, PIK3CA mutation showed a trend toward a significant adverse effect on OS with a pooled HR of 1.83 (95% CI, 1.05-3.20) in NSCLC patients treated with EGFR-TKIs (Figure 5C). Between-study heterogeneity was not significant; thus, the analysis was performed in the fixed-effect model (I2=26.9%; P=0.255).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Meta-analysis of the predictive value of PIK3CA mutation. (A) Forest plots of OR and 95% CI for ORR; (B) Forest plots of HR and 95% CI for PFS; and (C) Forest plots of HR and 95% CI for OS. OR, odds ratio; HR, hazard ratio.
Sensitivity analysis and publication bias of all above analyses was not performed because of the relatively limited eligible studies. Subgroup analysis was not conducted because of the relatively small size of included articles.
Discussion
EGFR inhibitor elicits multiple downstream effects, primarily moderated by RAS/RAF/MAPK and PI3K/AKT/mTOR signaling pathways. Rational use of target therapy requires the optimal selection of patients whose tumors are dependent on the activation of these two pathways. The predictive value of gene mutations on these two pathways downstream of EGFR for EGFR-TKI treatment is gradually recognized. This meta-analysis reveals an independent predictive value of K-ras and PIK3CA genetic status on EGFR-TKI therapy.
Coincident with previous report, our results again demonstrated that NSCLC patients harboring K-ras mutation had poor response to EGFR-TKIs. Exclusion of possible duplicate study reduced publication bias significantly and did not alter the pooled result, thus proving the stability of our result. More importantly, we quantitatively demonstrated that such patients had shorter PFS and OS compared with wild-type patients. Given that heterogeneity was zero across the studies in the analysis of the impact of K-ras mutation on PFS of NSCLC patients treated with EGFR-TKIs, a trim-and-fill method was applied to adjust publication bias. The adjusted pooled HR did not alter significantly the primary result, suggesting the dependability of our results. Slight heterogeneity was observed in the meta-analysis of the impact of K-ras mutation on the OS of NSCLC patients treated with EGFR-TKIs. Subgroup analysis showed that if K-ras mutation is concomitant with EGFR mutation, previous treatment and mutation detection method (Table 3) might affect the result. However, a negative effect of K-ras mutation on the OS of NSCLC patients with the EGFR-TKI treatment was observed in all subgroups. All these results indicated the adverse impact of mutant K-ras on the response and survival outcomes of NSCLC patients treated with EGFR-TKIs. This adverse effect has been proved in other cancers58.
Results of subgroup analysis of pooled HRs for OS of patients harboring K-ras mutation with EGFR-TKI treatment
Mutant PIK3CA proteins increase catalytic activity resulting in enhanced downstream signaling and oncogenic transformation in vitro59. Preclinical data showed that introducing activated PIK3CA mutations into EGFR-mutated lung cancer cell lines confers resistance to EGFR-TKIs60. Consistent with this result, our analysis revealed significantly shorter OS, poor ORR, and shorter PFS in PIK3CA mutant NSCLC patients treated with EGFR-TKIs.
The most common mutation of PIK3CA was found in exons 9 and 2061, corresponding to the helical and kinase domains, respectively. The predictive value of PIK3CA as a negative biomarker for anti-EGFR response in colorectal cancer differed in exons 9 and 2062. However, similar study in NSCLC was rarely reported in published articles, and no clear evidence was obtained to show that the impact of mutations in exons 9 and 20 of PIK3CA on anti-EGFR response differ in NSCLC. Thus, further analysis of the predictive value of these two exons separately with enlarged samples size is needed to achieve definite conclusion.
Slight heterogeneity was observed in the analysis of the impact of PIK3CA mutation. Although subgroup analysis could not be conducted because of insufficient data, some diversity on whether PIK3CA mutation was concomitant with EGFR mutation, mutation detecting method, and data extraction method was observed. Coexistence of PIK3CA mutations with EGFR is frequent in lung cancer15,63,64. However, the predictive value of PIK3CA to anti-EGFR treatment in EGFR mutant or wild-type NSCLC is ambiguous at present. The accuracy and specificity of different mutation detection methods also varied, which led to different false positive and false negative rates36. Although extracting time-to-event data according to Tierney was preferable, it failed to circumvent the potential biases associated with relying on published data for meta-analysis as mentioned by the authors. Therefore, despite the slight heterogeneity of the included studies in the analysis of the impact of mutant PIK3CA on the response and survival outcomes of NSCLC patients, our result would be consolidated by increasing sample size.
Despite our efforts to provide an accurate and comprehensive analysis, limitations of our meta-analysis should be addressed. First, most of the included studies were retrospective. Second, not all published studies presented adjusted estimates or had been adjusted by similar potential confounders. Third, limited studies presented PIK3CA mutation data, in which only four studies provided ORR information, two studies provided PFS information, and three studies provided OS information. Thus, increasing sample size of studies will further increase the creditability of adverse effect of PIK3CA mutation on clinical prognosis of NSCLC patients receiving EGFR-TKI treatment.
In conclusion, this meta-analysis indicated that K-ras mutation is probably a valuable predictive biomarker for assessing the clinical response and survival outcomes of NSCLC patients treated with EGFR-TKIs. More importantly, similar trends for PIK3CA mutation were shown in this meta-analysis, although the trends in ORR and PFS were not significant. Increasing sample size of studies will further increase the creditability of adverse effect of PIK3CA mutation on the clinical prognosis of NSCLC patients receiving EGFR-TKI treatment. Mutations of K-ras and EGFR are usually mutually exclusive, and coexistence of mutation in PIK3CA and EGFR is common. Thus, determining the status of K-ras and PIK3CA is valuable to distinguish the optimal patients who will benefit from EGFR-TKI treatment.
Acknowledgements
This work was supported by Key Projects in the National Science & Technology Pillar Program (Grant No. 2013ZX09303001, 2015BAI12B12, and 2015BAI12B15), National Natural Science Foundation of China (Grant No. 81472473 and 81272360), and Tianjin Municipal Commission of Science & Technology Key Research Program (Grant No.13ZCZCSY20300). We thank Dr. Wei-Jia Zhang from the Department of Medicine, Icahn School of Medicine at Mount Sinai for providing constructive suggestions for manuscript preparation.
Footnotes
Conflict of interest statement No potential conflicts of interest are disclosed.
- Received March 30, 2015.
- Accepted June 10, 2015.
- Copyright: © 2015 Cancer Biology & Medicine
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC BY) 4.0, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.
- 42.
- 43.
- 44.
- 45.
- 46.
- 47.
- 48.
- 49.
- 50.
- 51.
- 52.
- 53.
- 54.
- 55.
- 56.
- 57.
- 58.
- 59.
- 60.
- 61.
- 62.
- 63.
- 64.