

keywords
Introduction
In this paper we present a case of monocytic sarcoma of the vertebral canal with a review of relevant literature references. According to the extensive morphological and immunohistochemical analyses, monocytic sarcoma is one type of myeloid sarcoma, and can be diagnosed from extensive morphological and immunohistochemical analysis. Most cases of myeloid sarcomas are associated with acute, or chronic leukemia, or myelo-proliferative disorders, as well as monocytic sarcoma[1]. Rarely, the tumors may be identified before the diagnosis of any hematological malignancy[2,3] and most of them predict portend existing, or pending acute myeloid leukemia (AML). Myeloid sarcomas may occur in almost every part of the body[1,4], but spinal monocytic sarcomas are relatively uncommon.
Case Report
A 28-year-old male was admitted to our hospital complaining of progressive low back pain and numbness in his legs for 10 days, and bladder incontinence for 1 day. His medical history was unremarkable. Physical examination revealed no abnormality. Sensory system assessment revealed hypoesthesia below L4 and motor system examination revealed 2/5 paraparesis. He was unable to stand, or walk unassisted. Deep tendon reflexes were hyperactive and Babinski signs were bilaterally positive. Laboratory tests revealed a white blood cell count of 3.900/mm3, a hemoglobin level of 11.0 g/dl and a hematocrit of 38.2%. Magnetic resonance imaging (MRI) of the lumbar spine revealed a posterior epidural mass between T12 and L1 (Fig.1A~B).

Sagittal T1W (A), T 2 W (B) S Elumbar MR revealed a solid intraspinal lesion extradurally located between T12 and L1 lumbar vertebral levels and about 5 cm × 2cm × 2 cm in size.
High-dose (10 g/d) methylprednisolone was given initially, and an emergent T12-L1 laminectomy was performed to relieve the compression on the spinal cord. A soft and grayish tumor compressing the spinal cord was identified during surgery. Histologically the tumor was composed of a relatively uniform population of immature cells, most of which were monocaryon (Fig.2A). Cells with bright basophilia, occasionally granular cytoplasm, consistent with myeloid lineage were present. Immunohistochemical staining revealed the expressions of CD68, CD45, and lysozyme, but MPO, CD15 were not present (Fig.2 B~F). Furthermore, we found immature monoblasts in the blood (Fig.3A). The most important finding was the bone marrow biopsy results which were consistent with acute myelocytic leukemia. The results of bone marrow slides showed that bone marrow hyperplasia was supreme, and most of the myeloid cells were immature monoblasts (Fig.3B). The immunophenotypes of bone marrow were also consistent with myelocytic leukemia (Fig.4). According to results of immunhistochemistry, peripheral blood and bone marrow biopsy, the final clinical diagnosis was spinal monocytic sarcoma with acute monoblastic leukemia-M5b without any symptoms of leukemia. Ten days after surgery, he gradually gained strength in his lower extremities and bladder function was restored. Unfortunately, the patient refused standard chemotherapy; radiation therapy to the spinal axis and tumor base; and bone marrow transplantation. Four months later the patient presented the same symptom as prescribed. He later died of acute myelocytic leukemia.

A, Photomicrgraph showing neoplastic cells with small round and hyperchromatic nuclei proliferation in a diffuse pattern. Hematoxylin and eosin stain, original magnification × 40. B~F, Photomicrographs demonstrating positive immunohistochemical staining for CD68 (B),CD45 (C), Lysozyme (D), and negative for MPO (E), CD15 (F).
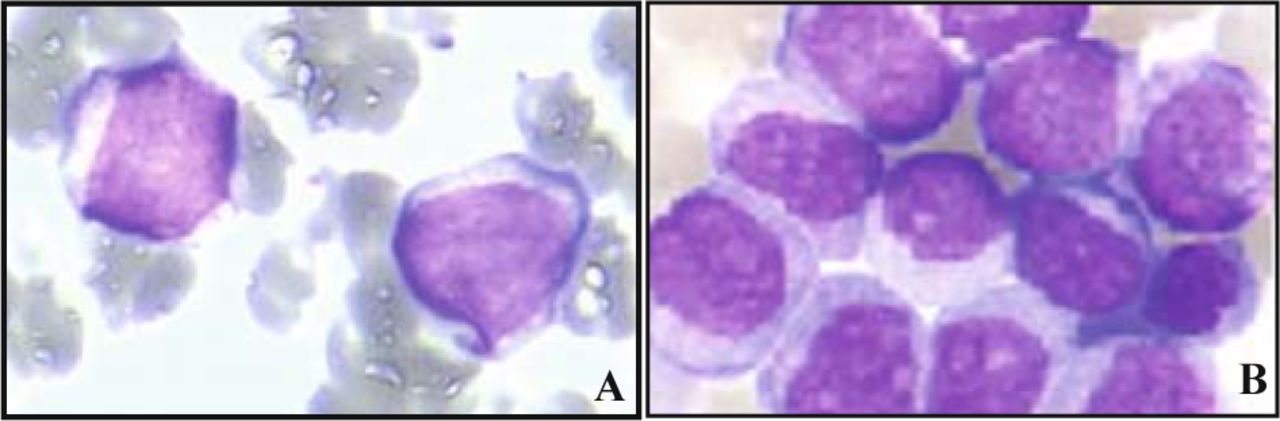
Photomicrgraph showing immature monoblasts in peripheral blood (A) and in bone marrow (B).

The immunophenotypes of bone marrow showing CD45, 41.43%; CD34, 1.54%; CD10, 2.42%; CD2, 0.28%; CD19, 0.63%;CD14, 0.20%; CD13, 9.49%; CD33, 77.65%; CD56, 31.68%. HLADR,95.22%; CD38, 6.38%; CD7, 0.94%; CD117, 44.38%; CD64, 80.14%; CD15, 96.07%.
Discussion
Myeloid sarcoma is a neoplasm composed of immature granulocytes, monocytes, or both, and many present at any extramedullary sites[5]. The neoplasm usually occurs in patients with acute myeloid leukemia, myelodysplastic, or myeloproliferative disorder. Myeloid sarcomas usually occur in the bones, skin, and lymph nodes. Bony involvement is most common in the orbit, sacrum, and ribs[6-8] and less often in the central nervous system and spinal cord[9]. With extensive morphological and immunohistochemical analyses, the myeloid sarcomas are classified into five types: i) immature granulocytic sarcoma (IGS); ii) differentiated granulocytic sarcoma (DGC); iii) monoblastic sarcoma (MBLS); iv) monocytic sarcoma (MS), and myelomonocytic sarcoma (MMS). These tumors are also morphologically and immunophenotypically analogous to their leukemic counterparts, as described in previous reports[10].
Monocytic sarcoma is one of myeloid sarcomas. It is a rare disease without any symptoms of leukemic disease, and has a poor prognosis. It is almost impossible to distinguish monoblastic sarcoma from granulocytic sarcoma and other types of small round cell tumors on the basis of morphological examination alone. Immunohistochemistry is necessary for a correct diagnosis [10,11].
The diagnosis of monocytic sarcoma is often difficult in myeloid sarcoma cases when the myeloblastic cells are poorly differentiated and the tumor lacks the characteristic color. The most common misdiagnoses included granulocytic sarcomas, large cell lymphoma, malignant lymphoma, reticulum cell lymphoma, and histiocytic lymphoma[7,12]. A diagnosis of monocytic sarcoma is not ruled out when bone marrow biopsy specimens show no evidence of leukemia infiltration[13].
Immunohistochemical study plays an essential role in obtaining a correct diagnosis of monocytic sarcoma. Immunopositivity for myeloperoxidase is specific for granulocytic differentiation, while CD68 (PG-M1)-positivity suggests monocytic differentiation without any symptom of leukemia. Detailed clinicopathologic correlation is also helpful[14]. MPO and CD117 are the most sensitive markers for myeloid differentiation while monocytic precursors are most strongly expressed by CD68 [15]. The tumor cells in all cases are positive for CD68 (KP1), CD68 (PGM1), lysozyme, and CD45. MPO, CD15, CD163, CD117, T and B cell markers are negative[11]. In our case, photomicrographs demonstrated positive immunohistochemical staining for CD68, CD45, lysozyme, and negative for MPO, CD15.
Treatment options include surgical decompression, chemotherapy, radiation therapy or any combination of these treatment methods [12,14,16]. Surgery is the first choice for cases of acute spinal cord compression. Pathological examination of the specimens from the mass is very important in diagnosis especially in cases without systemic evidence of leukemia [14,16]. Monocytic sarcomas are radiosensitive and are often treated by local radiotherapy and systemic chemotherapy. Newly diagnosed patients with isolated myeloid sarcomas are usually treated with aggressive chemotherapy as long as they have acute myelogenous leukemia. RT alone cannot reach a cure[12]. It is important to get the accurate histologic diagnosis is established initially for myeloid sarcomas and all isolated cases of myeloid sarcomas. Even though they may appear to be cured by resection, or irradiation. They should also be treated as soon as possible with intensive chemotherapy similar to that used to treat acute nonlymphoblastic leukemia[17].
- Received September 24, 2008.
- Accepted November 14, 2008.
- Copyright © 2008 by Tianjin Medical University Cancer Institute & Hospital and Springer
References
In this issue






{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.