Article Text

Abstract
BACKGROUND AND AIMS The mechanism of gastrointestinal damage (mucositis) induced by cancer chemotherapy remains uncertain. The aims of this study were to define the time course and mechanism of small intestinal damage following chemotherapy in humans.
METHODS Patients receiving chemotherapy underwent upper gastrointestinal endoscopy (a maximum of two per patient) with duodenal biopsy prior to chemotherapy and again at 1, 3, 5, and 16 days after chemotherapy. Tissue was taken for morphometry, disaccharidase assays, electron microscopy, and for assessment of apoptosis using the Tdt mediated dUTP-biotin nick end labelling (TUNEL) method. Villus area, crypt length, and mitotic index were measured by a microdissection technique.
RESULTS Apoptosis increased sevenfold in intestinal crypts at one day, and villus area, crypt length, mitotic count per crypt, and enterocyte height decreased at three days after chemotherapy. Disaccharidase activities remained unchanged. Electron microscopy showed increased open tight junctions of enterocytes at day 3, consistent with more immature cells. All indices improved by 16 days.
CONCLUSION Small intestinal mucositis is associated with apoptosis in crypts that precedes hypoplastic villous atrophy and loss of enterocyte height.
- chemotherapy
- mucositis
- small intestine
Abbreviations used in this paper
- TUNEL
- Tdt mediated dUTP-biotin nick end labelling
Statistics from Altmetric.com
Mucositis is a clinical term used to describe damage to mucous membranes that occurs after cancer chemotherapy.1 ,2 It occurs in 10–40% of patients and is clinically manifest by mouth symptoms such as oral pain and erythema, and gastrointestinal symptoms such as bloating, abdominal pain, and diarrhoea.1 ,2 There is no evidence that it is an inflammatory condition, as suggested by its designation. Most cytotoxic drugs induce gastrointestinal toxicity.3 ,4 The mechanism and exact anatomical distribution of non-oral mucositis have not been clearly defined. Mucositis has been attributed to the high physiological proliferation and turnover of cells in the small intestine that is affected by cancer chemotherapy.5-7 Both radiotherapy and chemotherapy in animal studies cause intestinal damage with apoptosis of intestinal crypts and crypt hypoplasia.4 It is important to confirm this sequence of events in humans, as the use of chemotherapy is potentially hazardous. Older studies of the effect of chemotherapy in humans found reduced crypt proliferation and reported occasional membrane bound bodies in crypts that would be compatible with apoptosis, although this process of cell death was not widely recognised at the time.5 ,8 The primary mechanism of mucositis could therefore be apoptosis that later leads to crypt hypoplasia. However, a recent paper by Pritchard and colleagues,9 studying the effects of 5-fluorouracil on mice, has shown that apoptosis is not necessarily predictive of subsequent crypt damage.
Apoptosis is known as programmed cell death, or cell suicide. It is not associated with inflammation, in contrast with necrosis. It is an active process in which there is rapid condensation of the nucleus and cytoplasm with preservation of organelles, followed by nuclear and surface budding to produce apoptotic bodies, which are phagocytosed intact and digested by normal cells.10 RNA and protein synthesis are required as it is active self-destruction rather than degeneration. Apoptotic cells occur predominantly in the lower (stem cell) region of the crypts with one apoptotic cell every five longitudinal crypt sections in normal small intestine.11The questions arise, does apoptosis increase in intestinal crypts after cancer chemotherapy in humans? And is there a direct relationship between apoptosis and histological damage?
The aims of this study were to investigate the time course and mechanism of intestinal damage in human patients receiving cancer chemotherapy. Apoptosis was investigated using the Tdt mediated dUTP-biotin nick end labelling (TUNEL) technique12 and electron microscopy, while intestinal damage was quantified using histomorphometry.
Subjects and methods
SUBJECTS
Patients were recruited from those with newly diagnosed malignancy who had not previously received chemotherapy, as well as those undergoing high dose chemotherapy and autologous blood stem cell transplantation. They had been referred to the Department of Haematology/Oncology at the Queen Elizabeth Hospital. There were 10 males and 13 females with a median age (range) of 45 (18–72) years. Standard dose chemotherapy was used in 13 patients and high dose chemotherapy in 10. Multiple drug regimens were used, with most agents being administered over 1–4 hours. The malignancies (number of patients) were: breast cancer (six), non-Hodgkin's lymphoma (five), multiple myeloma (two), non-small cell lung cancer (two), small cell lung cancer (one), cancer of the bladder (one), sarcoma (one), Hodgkin's disease (one), chronic myeloid leukaemia (one), oesophageal cancer (one), gastric cancer (one), and colorectal cancer (one). Numbers were not large enough to perform a subset analysis based on agents used.13 Patients were studied once prior to treatment and again at 1, 3, 5, or 16 days after chemotherapy. Clotting status was reviewed on the day of endoscopy by measuring INR and platelet count. No patient was rejected for endoscopy because of an abnormal clotting profile and no specific treatment, such as fresh frozen plasma or platelet infusion, was necessary. The study was approved by the Ethics of Human Research Committee of Queen Elizabeth Hospital and was carried out in accordance with the Declaration of Helsinki. Informed consent was obtained from each patient prior to enrolment in the study.
ENDOSCOPY AND DUODENAL BIOPSY
Patients were prepared in the normal manner for endoscopy, after a six hour fast. The upper gastrointestinal tract was inspected, and multiple biopsies were taken from the third part of the duodenum. Biopsies were fixed with shaking in Clarke's fixative (75%v/v ethanol:25% v/v glacial acetic acid) for morphometry. Villus area, crypt length, and mitotic count were measured using a microdissection technique.14 Further biopsies were placed in Carnoy's fixative to assess enterocyte height in haematoxylin-eosin sections, in 10% neutral buffered formalin for TUNEL assay, in 1.0% glutaraldehyde in 0.1 M sodium cacodylate buffer (pH 7.2) for electron microscopy to measure tight junctions, and others were taken for disaccharidase activities.
LIGHT MICROSCOPY
Intestinal morphometry
Duodenal biopsies were fixed in Clarke's fixative overnight and transferred to 70% alcohol until microdissection was performed. They were stained with Feulgen reagent and microdissected. At microdissection, small rows of villi and crypts are cut with a cataract knife and mounted as a wet film. By focusing up and down, a whole villus, crypt, and mitotic figures in the crypt can be easily visualised. Villus area was calculated using a trapezoid approximation as previously described.15 Crypt length and mitotic count per crypt were also recorded, with a minimum of 10 crypts per sample being counted.
Apoptotic count by TUNEL method
Apoptosis was detected in formalin fixed and paraffin embedded 4 μm sections by the TUNEL method.12 Briefly, sections were brought back to water and incubated with 20 μg/ml of proteinase K (P.6556, Sigma, Sydney, Australia) for four minutes at room temperature. Endogenous peroxidase was blocked by treating with 3% (v/v) hydrogen peroxide in methanol for 45 seconds. After washing, sections were incubated for 20 minutes at 37°C with TdT buffer consisting of 30 mM Tris (pH 7.2), 140 mM sodium cacodylate, 1 mM cobalt chloride, and 0.1% (w/v) bovine serum albumin. Reaction mixture was added consisting of 0.3 U/μl terminal transferase (No 252L, New England Biolabs, Beverley, Massachusetts, USA), 16.7 pmol biotin-16-2′-deoxyuridine-5′ phosphate (No 1093.070, Boehringer Mannheim/Roche, Castle Hill, Australia), and 0.05% bovine serum albumin in TdT buffer for 60 minutes at 37°C. The slides were dipped in phosphate buffered saline (pH 7.4) and placed in two changes of 300 mM sodium chloride and 30 mM sodium citrate for 15 minutes at room temperature. After washing three times (20 seconds each) in phosphate buffered saline, the biotin label was amplified by incubating using an avidin/biotin peroxidase technique (No PK-6102, Vector ABC Elite, Burlingham, California, USA) for 30 minutes at room temperature. Colour was developed with 1 mg/ml diaminobenzidine tetrachloride (D.5905, Sigma, Sydney, Australia)/0.015% (v/v) hydrogen peroxide for six minutes. The slides were counterstained with haematoxylin before mounting. Apoptotic cells per crypt were counted in 10 crypts and expressed as apoptotic bodies per crypt per 4 μm tissue section.
Enterocyte height
Enterocyte height was measured in haematoxylin-eosin sections of tissue fixed in Carnoy's fixative. Sections (5 μm) were examined under light microscopy at a magnification power of ×40 using a calibrated eyepiece. Enterocyte height of at least 10 cells in the mid-villus was recorded and the average calculated. Ten villi were counted per patient, and the results averaged.
ELECTRON MICROSCOPY
Duodenal tissue pieces (approximately 0.5 mm2) were fixed for at least one hour in a mixture of 1% glutaraldehyde and 10% formalin in 0.1 M sodium cacodylate buffer (pH 7.2). Tissue was post-fixed in 2% osmium tetroxide and stained en bloc in 2% uranyl acetate. Tissue was dehydrated through a graded series of alcohols (70%, 90%, 100%) and further processed through epoxypropane (100%), a 50/50 mixture of epoxypropane and Procure 812 resin (Electron Microscopy Sciences, Pennsylvania, USA), and two changes of Procure 812 resin. The tissue pieces were embedded in polythene capsules and cured overnight at 90°C. Survey sections were cut at approximately 2 μm and stained with toluidine blue. Duodenal villi were considered suitable for ultramicrotomy if they were clearly attached to lamina propria. Thin sections were cut at silver-gold colour (approximately 100 nm) and mounted on copper grids. Sections were stained with 2% uranyl acetate and Reynold's lead citrate, and examined with a Hitachi H-600 transmission electron microscope at a potential difference of 75 kV. Tight junctions were examined at a final magnification of 80 000. All specimens were randomised by a co-worker such that the examiner was blinded to the history of each specimen. Tight junctions were examined at sites where the luminal microvilli were considered perpendicular or near perpendicular to the axis of the electron beam. One hundred tight junctions per specimen were examined and scored as closed (normal), open, or oblique (unable to comment on the status of the tight junction due to obliquity of the junction in the plane of section) at the luminal surface. A tight junction was considered morphologically normal if there was no evidence of a gap between opposing cells at the luminal surface, and there was no visible gap between opposing leaflets of the tight junction.
DISACCHARIDASES
Disaccharidases were analysed in the Department of Tissue Pathology, Institute of Medical and Veterinary Science, as previously described and validated.16 Disaccharidases were expressed as micromoles disaccharide hydrolysed per minute per gram wet weight of tissue at 37°C. The 90% confidence intervals for lactase, sucrase, and maltase were 3–14, 6–26, and 13–44, respectively.
STATISTICS
Data are summarised as mean (SEM). Results were analysed using Peritz' F test, which is a robust test of comparison of group means, where group sizes are not identical.17
Results
SUBJECTS
There were no untoward complications in the 23 subjects. Eighteen had pre-chemotherapy biopsies, six had biopsies on day 1, eight on day 3, two on day 5, and seven on day 16 after chemotherapy. At endoscopy prior to chemotherapy, two patients were found to have gastritis withHelicobacter pylori infection, and one had oesophagitis. On day 1 after chemotherapy, two patients had gastritis and two had duodenitis. On day 3, three patients had developed oesophagitis, one had gastritis, and one had duodenitis. On day 5, one patient had oesophageal candidiasis, gastritis, and aphthous ulceration in the duodenum. There were no abnormal endoscopic findings in patients on day 16 after chemotherapy.
LIGHT MICROSCOPY
Morphology and morphometry
An example of changes in intestinal morphology before and three days after chemotherapy is shown in fig 1. This shows mild villous atrophy. Villus area and crypt length are given in fig 2. Villus area and crypt length decreased by 24% and 26%, respectively, at day 3 after chemotherapy and returned to pretreatment values by day 16. Changes in crypt proliferation are given in fig 3. Mitotic count decreased by 72% on day 3 after chemotherapy and returned to pretreatment values by day 16. There was no detectable reduction in mean (SEM) villus area between patients who received standard chemotherapy (0.264 (0.029) mm2, n=3) and those who received high dose chemotherapy (0.189 (0.040) mm2; n=5; NS).

Changes in intestinal morphology before (A) and at three days after (B) chemotherapy for cancer. (Original magnification ×156.)

Changes in villus area and crypt length before (Pre) and after chemotherapy for cancer. Data are given as mean (SEM).
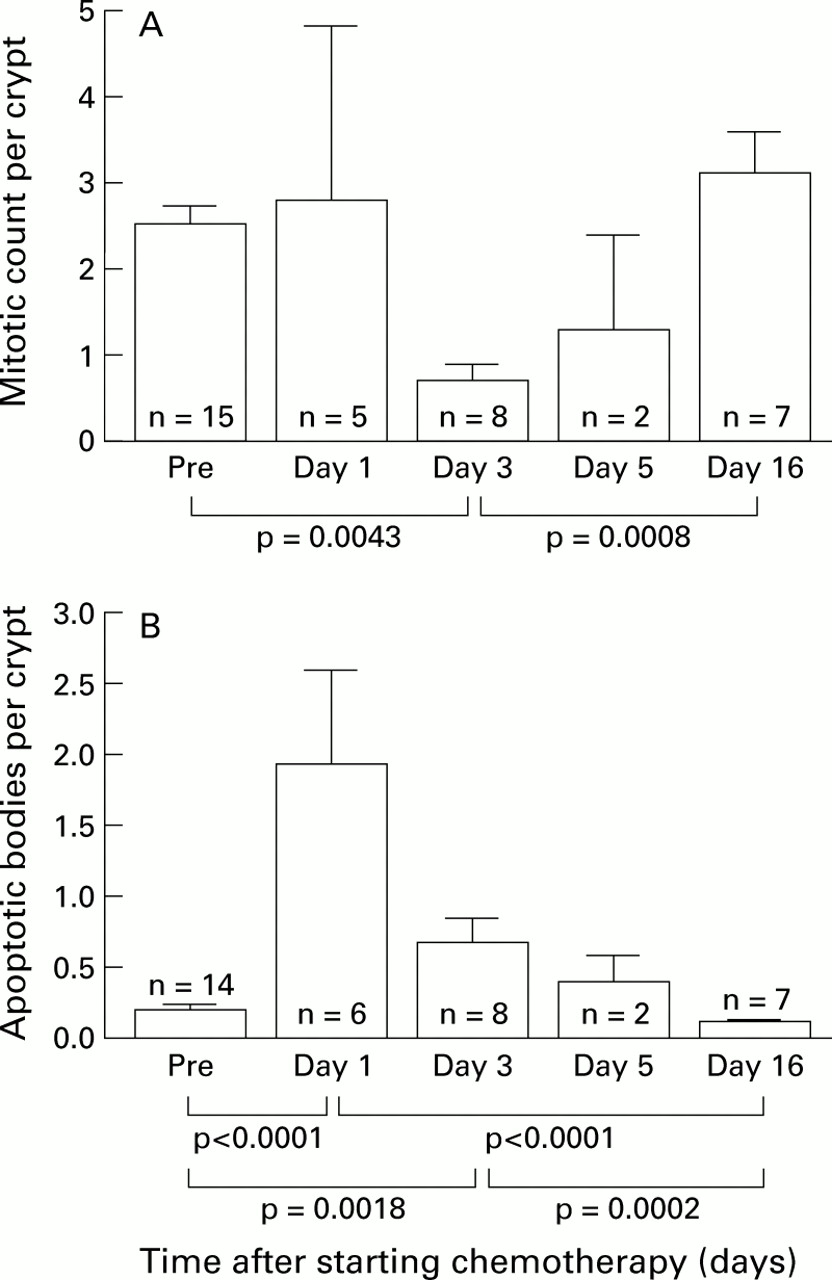
Changes in mitotic count per crypt (A) and apoptotic count per crypt per 4 μm section (B) before (Pre) and after chemotherapy for cancer. Data are given as mean (SEM).
Apoptosis
Changes in apoptotic bodies in intestinal crypts are given in fig3. Apoptotic bodies were increased by sevenfold at day 1, by 3.6-fold at day 3, and by twofold at day 5 after chemotherapy compared with pretreatment values. Thus the first histological effect of chemotherapy was early induction of apoptosis in intestinal crypts that preceded hypoproliferation. Figures 4 and 5 show light and electron micrographs of apoptotic epithelial cells on day 1 after chemotherapy. The pyknotic nucleus of the apoptosing cell is seen in the cytoplasm of an epithelial cell on electron microscopy.
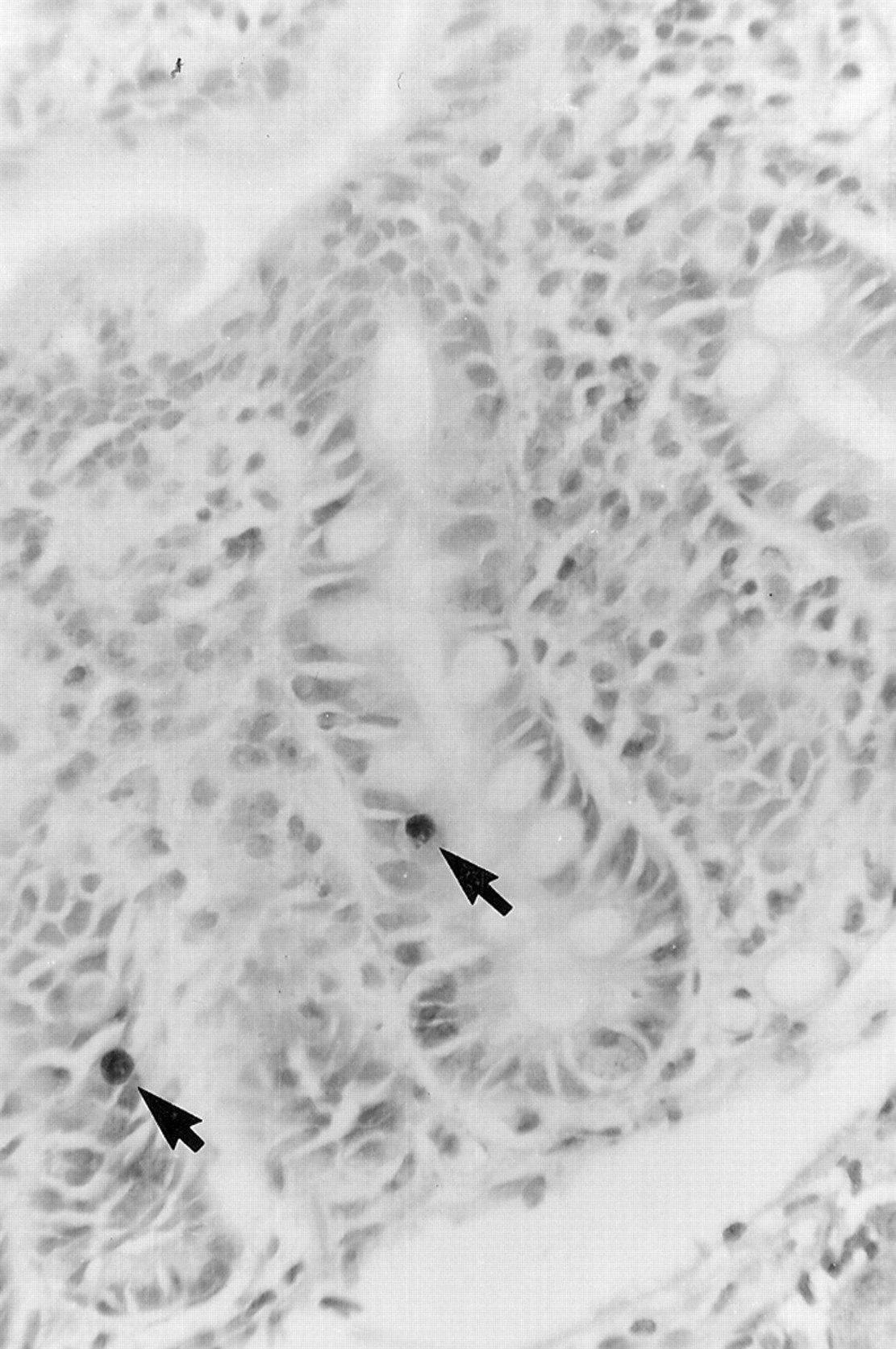
Light photomicrograph showing two apoptotic cells (arrows) in the crypt of the small intestine at one day after chemotherapy. Apoptosis was detected using the TUNEL technique. (Original magnification ×292.)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Electron micrograph of an apoptotic cell in the epithelial layer of the small intestinal crypt at one day after chemotherapy. The arrow indicates an apoptotic cell with a pyknotic nucleus. (Original magnification ×12 000.)
Enterocyte height
Mean (SEM) enterocyte height was 31.9 (1.1) μm prior to treatment, which decreased significantly to 28.2 (1.6) μm at day 3 (p=0.018), and returned to pretreatment values of 32.5 (1.3) μm by day 16.
Electron microscopy
Mean (SEM) percentage of open tight junctions prior to treatment (n=17) and on days 1 (n=5), 3 (n=8), 5 (n=2), and 16 (n=7) after treatment were 38.9 (4.4)%, 54.3 (1.7)%, 63.3 (6.0)%, 59.0 (20.1)%, and 46.6 (8.1)%, respectively. These changes are consistent with repopulation of the villus with immature cells at day 3 after chemotherapy.
DISACCHARIDASES
Disaccharidase activities are given in table 1. Disaccharidases showed no significant change before or after chemotherapy.
Disaccharidases in patients before and three and 16 days after chemotherapy for cancer. Activity is expressed as micromoles disaccharide hydrolysed per minute per gram wet weight of tissue at 37° C. Data are given as mean (SEM)
Discussion
The earliest effect of chemotherapy in our study was a sevenfold increase in apoptosis in intestinal crypts at one day after chemotherapy for cancer. Apoptosis was confirmed on electron microscopy. It was followed at three days by a reduction in villus area, crypt length, mitotic count, and enterocyte cell height. All measures returned to pretreatment values by day 16 after chemotherapy. Although this finding of early induction of apoptosis in intestinal crypts might be expected on the basis of rodent studies,3 ,4 these animal studies differed markedly in the intensity of cytotoxic chemotherapy administered.
A variety of studies of chemotherapy on the small intestine have shown crypt hypoplasia in humans and rodents.3-8 These established the notion that chemotherapy damages the small intestine because it is a rapidly dividing tissue. Trier showed reduced crypt proliferation 3–48 hours after methotrexate treatment of human subjects; Ijiri and Potten showed that all cytotoxic drugs in animals cause both apoptosis and crypt hypoplasia.3-5 The present study showed that apoptosis preceded intestinal crypt hypoplasia after chemotherapy in human cancer patients. It is interesting that older studies of the effects of chemotherapy on the intestine observed discrete spherical bodies in crypts, and pyknotic nuclear material in crypts that could have been apoptotic bodies.5 These studies were performed before apoptosis was widely recognised as a pathophysiological process. We have extended our human study to an animal study of rats implanted with breast cancer and treated with methotrexate (unpublished data, 1999). This has shown an early peak of apoptosis from six hours to two days after chemotherapy that precedes morphometric changes of hypoplastic villous atrophy in the absence of severe mucosal destruction that was previously associated with animal studies. Presumably, apoptosis reduces available stem cells that can proliferate.10 ,18
Potten and coworkers found that apoptosis was markedly induced in intestinal crypts of mice after irradiation or combined radiotherapy and chemotherapy.11 ,19 The difficulty of extending these findings from animal studies to human patients could be the difference in severity of intestinal damage, but genetic differences can lead to differences in susceptibility to mucosal damage, even within species. This present study showed that chemotherapy induced apoptosis of intestinal crypts in human patients without mucosal destruction but with morphometric reduction in crypt size and proliferation. This would be expected, as chemotherapy acts on malignant cells by inducing apoptosis that is seen exclusively in vitro, although necrosis also occurs in solid tumours to a lesser extent in vivo.20 ,21
Pritchard and colleagues9 have shown that 5-fluorouracil causes apoptosis in small and large intestinal crypts in mice, but that it is not dose dependent. Histopathological changes required higher doses of 5-fluorouracil than apoptosis, and were associated with p53 dependent inhibition of cell cycle. Doses of chemotherapy used in our human study caused both apoptosis and histopathological changes, and the role of p53 needs further investigation.
The question also arises why mucositis involves the small rather than the large intestine? In the small intestine the stem cells are believed to be located at cell positions 3–5, but in the colon they are believed to be located at positions 1–2. Potten and colleagues have shown that in the small intestine, apoptosis tends to be highest at positions 3–5, thus deleting stem cells. Apoptosis in the colon also occurs at levels 3–5, thus sparing the differently located stem cells.19 Mucositis is becoming a limiting factor for increasing the dose of chemotherapy now that bone marrow toxicity can be managed by supportive care, blood transfusion, and colony stimulating factors. The present human study and our unpublished animal study further illustrate the fundamental dilemma that chemotherapy acts by inducing apoptosis (and necrosis in tumours) but also induces apoptosis in the gastrointestinal tract. Treatment must therefore prevent apoptosis in the gastrointestinal tract (and other vulnerable sites) but must not prevent apoptosis in neoplastic tissue. This could explain why specific treatment of intestinal mucositis until now has not been successful.
We conclude that chemotherapy for cancer induces apoptosis in crypts of the small intestine that precedes hyoplastic villous atrophy. Intestinal hypoplasia reaches a nadir at three days after chemotherapy. This corresponds with our previous observation of peak gastrointestinal symptoms and functional impairment of monosaccharide absorption and increased intestinal permeability from days 3 to 7 after high dose chemotherapy.22
Acknowledgments
We thank Drs R E Sage, B M Dale, J E Norman, D Kotasek, and R M Green for allowing us to study patients under their care, and acknowledge the helpful assistance of the nursing staff of both the Haematology/Oncology and Endoscopy Units, Queen Elizabeth Hospital. This study was supported by the Anti-Cancer Foundation of the Universities of South Australia, by the University of Adelaide and by the Queen Elizabeth Hospital Research Foundation. Dr Keefe received a research associateship from the Anti-Cancer Foundation of the Universities of South Australia.
Abbreviations used in this paper
- TUNEL
- Tdt mediated dUTP-biotin nick end labelling