
Abstract
Background
In 2004, docetaxel was shown to prolong the overall survival (OS) of patients with metastatic castration-resistance prostate cancer (mCRPC). Since 2010, five new systemic therapies have been shown to prolong OS in men with mCRPC. We sought to evaluate the aggregate impact of these newer therapies on the OS of patients with mCRPC.
Methods
Two cohorts of patients diagnosed with mCRPC between 2004 and 2007, treated with drugs used in the limited treatment era only (A), and between 2010 and 2013, treated also with newer therapies (B), were identified from the Dana-Farber Cancer Institute database. The analysis endpoint was OS within 5 years after mCRPC diagnosis. Kaplan–Meier method assessed time-to-event distributions with median (95% confidence interval (CI)). A piece-wise regression model assessed the association between endpoint and treatment cohorts with estimate of hazard ratio (HR) with 95% CI within two time segments in univariate and multivariable analyses adjusting for relevant covariates.
Results
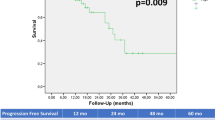
Compared to cohort A (n = 318), cohort B (n = 272) patients in newer therapy era demonstrated an OS advantage (2.8 vs. 2.2 years) with a 41% decreased risk of death (HR = 0.59; 95% CI, 0.47–0.74; P < 0.0001), and a 3-year OS rate of 46% vs. 33%. This benefit was accentuated (median OS 2.7 vs. 2.1 years; HR = 0.46; 95% CI, 0.32–0.67; P < 0.0001) in patients who initially presented with de-novo metastatic disease (de-novo). On multivariable analysis, longer OS was associated with cohort B vs. A and performance status 0 vs. 1.
Conclusions
Using a single-institution registry, mCRPC patients treated since 2010 had a significant survival improvement vs. those treated before 2010. Although the median survival was only modestly improved and less than predicted when simply adding each newer drug survival advantage, the cumulative benefit from the new therapies was more pronounced in longer-term survivors and de-novo patients.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 4 print issues and online access
$259.00 per year
only $64.75 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout

Similar content being viewed by others


References
National Cancer Institute: Surveillance, Epidemiology, and End Results Program: Cancer Stat Facts: Prostate Cancer. https://seer.cancer.gov/statfacts/html/prost.html.
Scher HI, Solo K, Valant J, Todd MB, Mehra M. Prevalence of prostate cancer clinical states and mortality in the United States: estimates using a dynamic progression model. PLoS One. 2015;10:e0139440.
Tannock IF, de Wit R, William RB, Horti J, Pluzanska A, Chi KN, et al. Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer. N Eng J Med. 2004;351:1502–12.
Petrylak DP, Tangen CM, Hussain MHA, Lara PN Jr, Jones JA, Taplin ME, et al. Docetaxel and estramustine compared with mitoxantrone and prednisone for advanced refractory prostate cancer. N Engl J Med. 2004;351:1513–20.
Kantoff PW, Higano CS, Shore ND, Berger ER, Small EJ, Penson DF, et al. Sipuleucel-T immunotherapy for castration-resistant prostate cancer. N Engl J Med. 2010;363:411–22.
de Bono JS, Oudard S, Ozguroglu M, Hansen S, Machiels JP, Kocak I. et al. Prednisone plus cabazitaxel or mitoxantrone for metastatic castration-resistant prostate cancer progressing after docetaxel treatment: a randomised open-label trial. Lancet. 2010;376:1147–54.
de Bono JS, Logothetis CJ, Molina A, Hansen S, Machiels JP, Kocak I, et al. Abiraterone and increased survival in metastatic prostate cancer. N Engl J Med. 2011;364:1995–2005.
Ryan CJ, Smith MR, de Bono JS, Molina A, Logothetis CJ, de Souza P, et al. Abiraterone in metastatic prostate cancer without previous chemotherapy. N Engl J Med. 2013;368:138–48.
Scher HI, Fizazi K, Saad F, Taplin ME, Sternberg CN, Miller K, et al. Increased survival with enzalutamide in prostate cancer after chemotherapy. N Engl J Med. 2012;367:1187–97.
Beer TM, Armstrong AJ, Rathkopf DE, Loriot Y, Sternberg CN, Higano CS, et al. Enzalutamide in metastatic prostate cancer before chemotherapy. N Engl J Med. 2014;371:424–33.
Parker C, Nilsson S, Heinrich D, Helle SI, O'Sullivan JM, Fosså SD. et al. Alpha emitter radium-223 and survival in metastatic prostate cancer. N Engl J Med. 2013;369:213–23.
Chaumard-Billotey N, Chabaud S, Boyle HJ, Helle SI, O’Sullivan JM, Fosså SD, et al. Impact of news drugs in the median overall survival of patients with metastatic castration resistant prostate cancer (mCRPC). J Clin Oncol. 2013;31(Suppl 15): e16096–e16096 (abstract16096).
Veccia A, Caffo O, Burgio SL, di Lorenzo G, Ortega C, Scognamiglio F, et al. Impact of new agents (NAs) on post-docetaxel (DOC) survival of octogenarians with metastatic castration resistant prostate cancer (mCRPC) patients (pts): Results of an Italian multicenter retrospective study (DELPHI study). J Clin Oncol. 2015;33(Suppl 15):e16017–e16017 (abstract 16017).
Caffo O, Kinspergher S, Maines F, di Lorenzo G, Ortega C, Scognamiglio F, et al. Impact of new agents (NAs) on survival of metastatic castration-resistant prostate cancer (mCRPC) patients (pts): A single-Institution retrospective analysis. J Clin Oncol. 2018;36(Suppl 6):323–323 (abstract 323).
Bandini M, Pompe RS, Marchioni M, Zaffuto E, Gandaglia G, Fossati N, et al. Improved cancer‑specific free survival and overall free survival in contemporary metastatic prostate cancer patients: a population‑based study. Int Urol Nephrol. 2018;50:71–78.
Lorente D, Fizazi K, Sweeney C, de Bono JS. Optimal treatment sequence for metastatic castration-resistant prostate cancer. Eur Urol Focus. 2016;2:488–98.
Mezynski J, Pezaro C, Bianchini D, Zivi A, Sandhu S, Thompson E, et al. Antitumour activity of docetaxel following treatment with the CYP17A1 inhibitor abiraterone: clinical evidence for cross-resistance? Ann Oncol. 2012;23:2943–7.
Loriot Y, Bianchini D, Ileana E, Sandhu S, Patrikidou A, Pezaro C, et al. Antitumour activity of abiraterone acetate against metastatic castration-resistant prostate cancer progressing after docetaxel and enzalutamide (MDV3100). Ann Oncol. 2013;24:1807–12.
Noonan KL, North S, Bitting RL, Armstrong AJ, Ellard SL, Chi KN. Clinical activity of abiraterone acetate in patients with metastatic castration-resistant prostate cancer progressing after enzalutamide. Ann Oncol. 2013;24:1802–7.
Gravis G, Boher JM, Chen YH, Liu G, Fizazi K, Carducci MA, et al. Burden of metastatic castrate naive prostate cancer patients, to identify men more likely to benefit from early docetaxel: further analyses of CHAARTED and GETUG-AFU15 Studies. Eur Urol. 2018;73:847–55.
Gravis G, Boher JM, Joly F, Soulié M, Albiges L, Priou F, et al. Androgen deprivation therapy (ADT) plus docetaxel versus ADT alone in metastatic non castrate prostate cancer: impact of metastatic burden and long-term survival analysis of the randomized phase 3 GETUG-AFU15 Trial. Eur Urol. 2016;70:256–62.
Francini E, Gray KP, Xie W, Shaw GK, Valença L, Bernard B, et al. Time of metastatic disease presentation and volume of disease are prognostic for metastatic hormone sensitive prostate cancer (mHSPC). Prostate. 2018;78:889–95.
Scher HI, Morris MJ, Stadler WM, Higano C, Basch E, Fizazi K, et al. Trial design and objectives for castration-resistant prostate cancer: updated recommendations from the Prostate Cancer Clinical Trials Working Group 3. J Clin Oncol. 2016;34:1402–18.
Grambsch P, Therneau T. Proportional hazards tests and diagnostics based on weighted residuals. Biometrika. 1994;81:515–26.
Acknowledgements
Author contributions
Conception and design: EF, KPG, and CJS; collection and assembly of data: EF, GKS, CPE, AAH, and CEP; data analysis and interpretation: EF, KPG, PWK, M-ET, and CJS; manuscript writing: all authors; final approval of the manuscript: all authors; accountable for all aspects of the work: all authors.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
EF has been sponsored for travel, accommodations, and expenses by Janssen-Cilag. AAH has participated in advisory boards for Roche and received compensation. PWK has consulted or participated in advisory boards for Astellas, Bayer, Genentech, Janssen-Cilag, Merck, Sanofi, Dendreon, Medivation/Astellas, and Pfizer and received compensation; he also received grants or funding from Bayer, Dendreon, Genentech/Roche, and Medivation/Astellas, and has been sponsored for travel, accommodations, expenses by Sanofi. M-ET has consulted or participated in advisory boards for Janssen-Cilag and Medivation and received compensation: she also received grants or funding by Janssen-Cilag and Medivation, Travel, and has been sponsored for travel, accommodations, expenses by Sanofi. CJS has consulted or participated in advisory boards for Astellas, Bayer, Genentech, Janssen-Cilag, Pfizer, and Sanofi, and received compensation: he also received grants or funding by Astellas, Janssen-Cilag, Sotio, and Sanofi. KPG, GKS, CPE, and CEP declare that they have no conflict of interest.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Francini, E., Gray, K.P., Shaw, G.K. et al. Impact of new systemic therapies on overall survival of patients with metastatic castration-resistant prostate cancer in a hospital-based registry. Prostate Cancer Prostatic Dis 22, 420–427 (2019). https://doi.org/10.1038/s41391-018-0121-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41391-018-0121-2
This article is cited by
-
VSSP-activated macrophages mediate senescence and tumor inhibition in a preclinical model of advanced prostate cancer
Cell Communication and Signaling (2023)
-
Longitudinal change in castration-resistant prostate cancer biomarker AST/ALT ratio reflects tumor progression
Scientific Reports (2023)
-
Low hemoglobin and PSA kinetics are prognostic factors of overall survival in metastatic castration-resistant prostate cancer patients
Scientific Reports (2023)
-
Dendritic cell-based vaccine prolongs survival and time to next therapy independently of the vaccine cell number
Biology Direct (2022)
-
Editor’ summary: A paradigm shift in castration-resistant prostate cancer management
Prostate Cancer and Prostatic Diseases (2022)
