

Abstract
OBJECTIVE To explore the clinical and therapeutic effects of cervical plexus reinnervation for infiltrated or injured unilateral recurrent laryngeal nerve (URLN).
METHODS Functional neck dissection for removal of differentiated thyroid carcinoma (DTC) in patients was performed, in which cervical plexus reinnervation was adopted for patients with stage I disease and URLN with injury or with tumor invasion. Outcomes of surgery were evaluated by examination under fibrolaryngoscope, and the patients’ voices were evaluated before and aft er surgery.
RESULTS All cases were followed up for 3 mon-2 years (average 8 mon). Abductory motion of the vocal cords of 15 patients was completely or partly restored, but 3 patients’ vocal cords were immovable. The recovery rate of abductory motion of the paralyzed vocal cords was 83.33% (15/18). The function of phonation in the 16 patients was restored to normal or near normal limits, and their hoarseness was improved significantly.
CONCLUSION Cervical plexus-URLN reinnervation should be considered when treating patients with unilateral vocal cord paralysis. Removing the tumor simultaneously with cervical plexus reinnervation during surgery for repair of unilateral recurrent laryngeal nerve injury was convenient and easy to perform with less functional damage compared with other methods of reinnervation. The abductory motion of vocal cord could be satisfactorily restored by this reinnervation. Surgical performance skills and application of neurotrophic drugs were important for the success of the surgery.
keywords
Introduction
Recurrent laryngeal nerve (RLN) paralysis is one of the major complications in thyroid surgery, resulting in hoarseness which not only affects patients’ quality of life, especially of professionals who rely on their voice, but also leads to dyspnea or life-threatening glottal obstruction when bilateral recurrent laryngeal nerves have been jeopardized[1-4]. For decades, different treatment options have been available for the management of unilateral vocal cord paralysis. A series of studies have shown that adductory motion of paralyzed vocal cord is restored by implantation of the ansa cervicalis, hypoglossal nerve or phrenic nerve for RLN reinnervation[5-7]; however the surgery has some disadvantages such as loss of functional movement of the tongue and difficulty in deciding the appropriate length or diameter of donor nerve for reinnervation. Therefore, an ideal nerve graft is the key-point in reinnervation for an RLN deficit.
During the process of functional neck dissection for patients with DTC, the accessory nerve, sternocleidomastoid muscle, internal jugular vein, and branches of the cervical plexus such as the great supraclavicular nerves are preserved routinely. This operation affects little of the sensation of the shoulder, and concurrently, the preserved cervical plexus is used to restore the function of the recurrent laryngeal nerve when injured or invaded by tumor. The surgeries we have performed have been successful. In the following, we describe what we have learned from doing the surgery on patients with unilateral vocal cord paralysis.
Patients and Methods
Patients
From May 2005 to April 2007, 18 thyroid carcinoma patients, with symptoms induced by unilateral vocal cord paralysis, were admitted to the Department of Head & Neck Tumors at Tianjin Medical University Cancer Institute & Hospital. Laryngoscopic examination of the vocal cords was routinely performed prior to surgery, and it showed that the involved vocal cord was either fixed in the paramedian or median position upon aspiration. The left vocal cord was paralyzed in 10 patients and the right in 8. Among the different causes of recurrent laryngeal nerve injury, there were 13 patients whose RLN was invaded or encased by tumor, and 5 cases which had complete recurrent laryngeal nerve injury during a previous thyroid surgery performed at another hospital. Among the 18 patients, 1 was male and 17 were female with a median age of 45.6 years ranging from 22 to 51. All patients were confirmed as having cervical nodal metastases through clinical examination and all received functional neck dissection. Twelve of the cases received primary cervical plexus reinnervation because of the URLN invasion, and 6 cases received secondary cervical plexus reinnervation for the injured URLN caused by the previous surgery. Surgery was performed on all 18 patients by the same surgeon under general anesthesia.
Surgical procedures
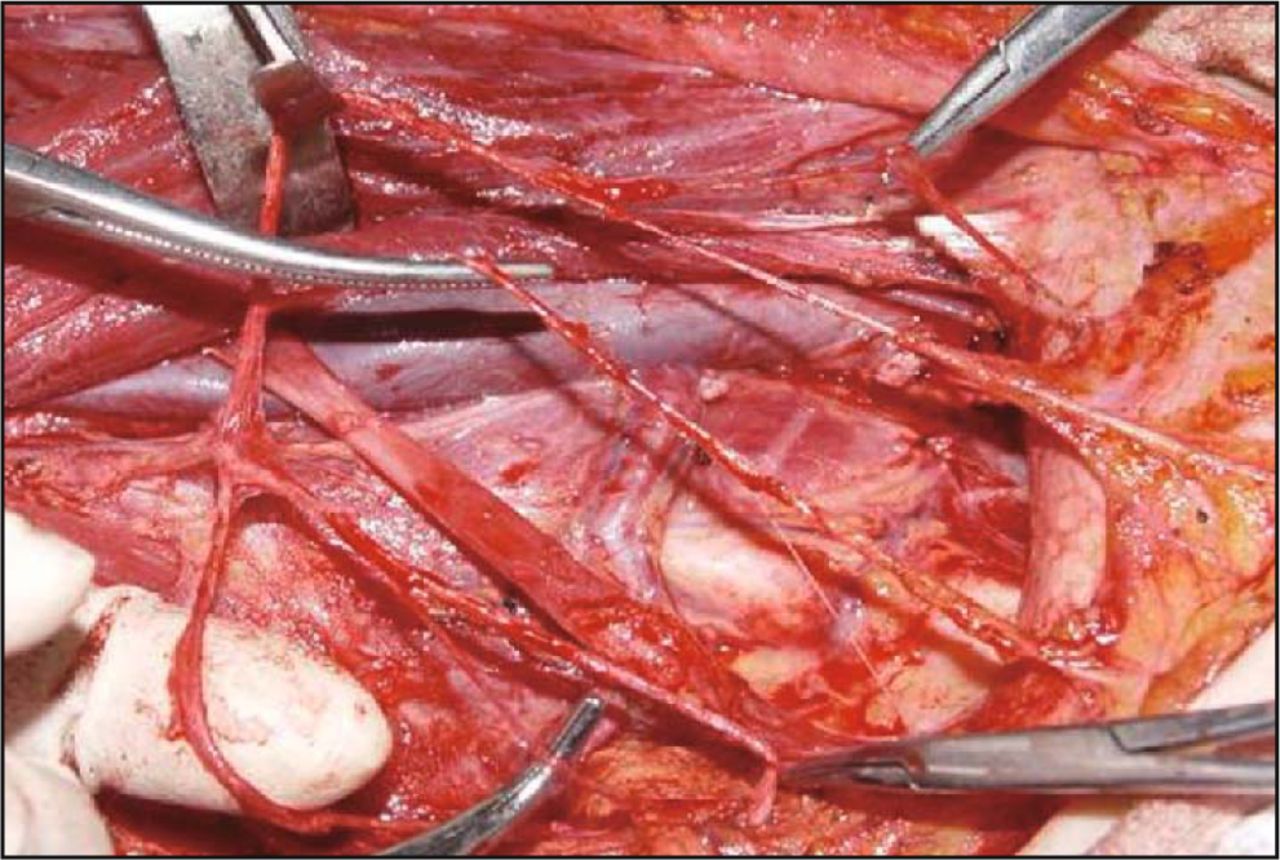
The surgical procedure of cervical plexus-RLN reinnervation was performed as follows. During the functional neck dissection of DTC, branches of the cervical plexus such as the great auricular nerve, and the supraclavicular nerves, which were not invaded by tumor, were preserved. Then the proximal part of the RLN which was invaded by tumor or injured previously was dissected until it was felt to be clear. Then the ends of RLN were trimmed to minimize the distal stump so as to promote early innervation. After preparing the RLN, the cervical plexus, which was selected appropriately (appropriate length and diameter) as a free nerve flap, was then freely used at the point where it was needed to rebuild nerve conduction (Fig. 1). The ending of the graft nerve was trimmed to match the stump of the RLN. The 2 nerve ends were freshened prior to placing 3 or 4 interval stitches of 5-0 absorbable suture, using micro-surgical instruments. During the operation, the RLN was transposed superiorly and positioned to the cut end of the cervical plexus to provide a tension-free anastomosis, and, concurrently, to ensure the correct conduction of the nerve signal (Fig. 2). Meanwhile, during surgery, the RLN and the graft nerve were kept moist by applying normal saline and twisting or rubbing of the nerves or the graft nerve were avoided. Neurotrophic drugs were administered routinely following the surgery.
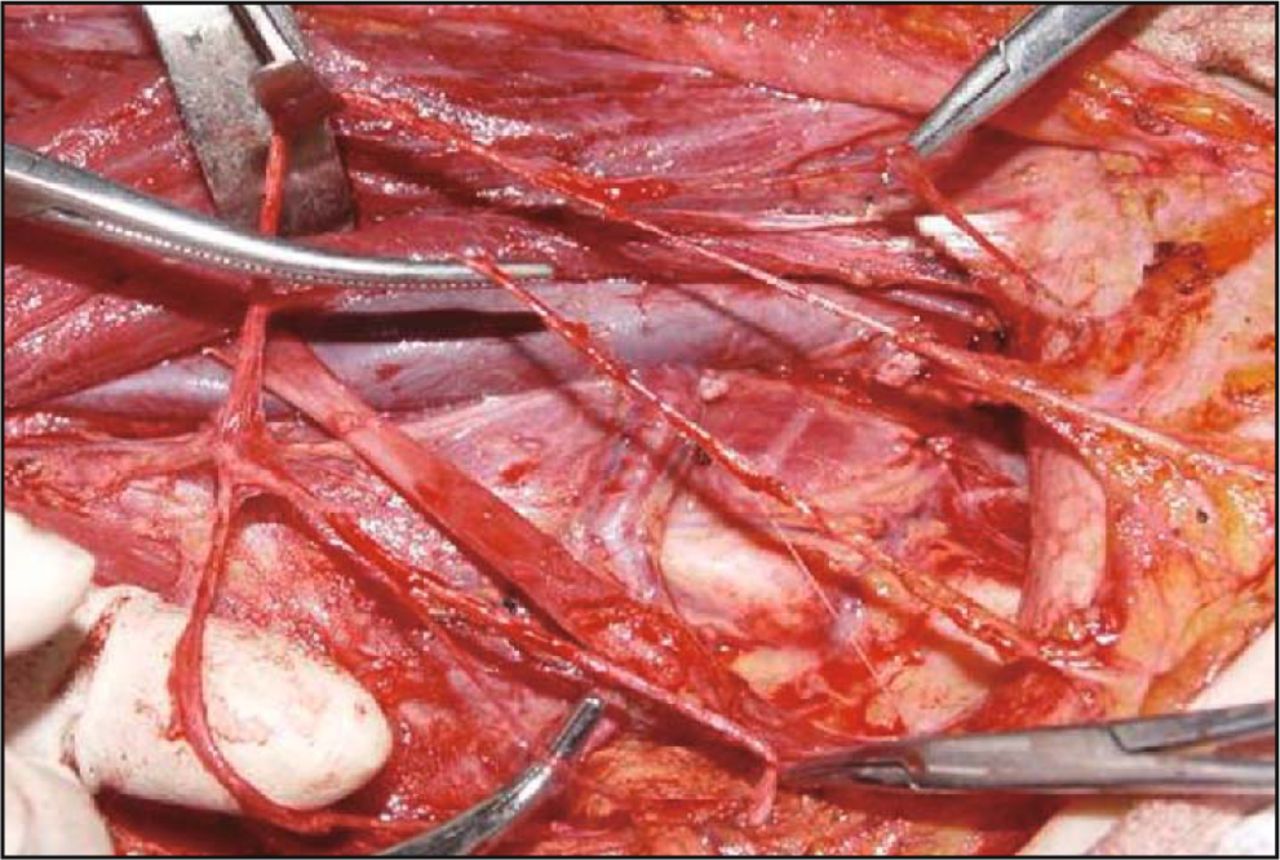
Preserved cervical plexus during surgery.

Cervical plexus-RLN reinnervation.
Evaluation of the effects of the surgery
Patients were followed up per 3 months postoperatively to check the movement of the vocal cords and the space of the glottal gap under the laryngofiberscope. Subjective ratings of aspiration and voice quality were made based on patient reports. The evaluation criteria for the surgery effects were as follows: Healing-the voice becomes normal or the paralyzed vocal cord has completely restored abductory and adductory motion. Effective-the hoarseness is improved or the paralyzed vocal cord has partly restored abductory or adductory motion. Ineffective-the hoarseness or the abductory and addutory motion of the paralyzed vocal cord is not improved.
Ethical permission
All patients involved in this study were required to fill out a consent form before participating in this study, which was approved by the Medical Ethics Committee in the hospital. Any information regarding the participants will be kept confidential strictly.
Statistical analysis
To test the curative effect of different types of cervical plexus reinnervation for recurrent laryngeal nerve injury, group differences were assessed using the Fisher exact tests for categorical data in SPSS13.0. A P value of < 0.05 was considered statistically significant.
Results
Patient perception survey
During a median follow-up of 8 mon with a range of 3-24 months, attempts were made to contact all 18 patients, and no patients were lost to follow up. The average time of patient perception of voice improvement and of recording of clinical signs and symptoms after reinnervation was 5 mon.
Laryngofiberoscopy
All of the 18 cases were followed up for more than 3 mon-2 years after the operation. The entirely or partially restored abductional or adductional movement of the vocal cords occurred in 15 cases (83.33%, 15/18) and their glottal gap amplitude ranged from 3 mm to 8 mm. We also found that the patients with a history of hoarseness before surgery lasting for less than 3 months (92.30%, 12/13) or more than 3 months (60%, 3/5) had a different restoration rate of the paralyzed vocal cord. The patients with a history of hoarseness before the surgery lasting for less than 3 months had a higher restoration rate of the paralyzed vocal cord than the patients with a longer history of hoarseness. In the remaining 3 cases, their vocal cord movement was not restored, and the vocal cord that was paralyzed was still in a paramedian position. The appearance of vocal cord abduction during inspiration was observed 1-3 months after reinnervation.
Voice evaluation
Subjective ratings of voice quality (normal, improved, not improved or with degeneracy) were made postoperatively based on patient reports. The phonation of 16 patients was restored to normal or near normal, and their hoarseness improved significantly. Of the 18 cases, there were 5 patients whose voice became normal, 11 patients whose voice improved and 3 patients whose voice was not improved. The effective rate of the surgery was 83.33% (15/18). In the cervical plexus reinnervation operations performed on the 18 patients, the surgical procedure in 14 cases used the deep branch of the cervical plexus as the graft nerve, and 4 cases used the superficial branch for the graft nerve. The effective rate of the restoration was 92.86% and 50%, respectively (Table 1).
The effect of cervical plexus reinnervation of the recurrent laryngeal nerve in 18 cases.
Discussion
The recurrent laryngeal nerves are vulnerable to becoming involved by primary thyroid carcinoma with extrathyroidal invasion because of their proximity to the thyroid gland. Recurrent laryngeal nerve injury caused by thyroid surgery, radical neck dissection, and other neck surgeries or trauma remains a source of morbidity in patients. The incidence of injury to the RLN during such operations varies from 0.3% to over 13%. Postoperative vocal cord paralysis still occurs in as many as 3%–4% of patients who have benign thyroid disease undergoing thyroid surgery[8,9]. This complication leads to many inconveniences for the life of the patients. Therefore, strategies that repair RLN injury are of great interest. The pioneering work of Elsberg demonstrated that a foreign nerve may reinnervate a denervated muscle fiber, even if they were dissimilar[10]. This study used the cervical plexus which was normally to be dissected in the neck dissection of DTC to reinnervate the unilateral recurrent laryngeal nerve which was injured or invaded. The results of the study showed a good outcome.
The benefits of using the cervical plexus as the donor for reinnervation
Different treatment options are available for the management of unilateral vocal cord paralysis, which include the ansa cervicalis, the hypoglossal nerve or the phrenic nerve as the graft for recurrent laryngeal nerve reinnervation[5-7]. These methods have several advantages in treating vocal cord paralysis, including the potential of restoring a normal or near normal voice without changing vocal cord pliability, which is the first factor to consider when selecting a treatment[11,12]. Additionally, these methods could prevent the progressive loss of thyroarytenoid muscle tone and bulk typically seen with vocal cord denervation, which can limit the long-term results of traditional laryngoplasty techniques i.e. the position of the cord changes over time[13,14]. Furthermore, patients receiving the reinnervation still have a chance to undergo other types of laryngoplasty techniques in the future if the reinnervation fails. For these reasons, some surgeons would like to select reinnervation as their first choice in the management of unilateral vocal cord paralysis. These methods are effective in improving the paralyzed vocal cord but all donor nerves have many deficiencies. For example, when using hypoglossal nerve-RLN reinnervation, the motion of tongue would be affected after operation and the patient’s quality of life would decline. As a part of the spinal nerve, the cervical plexus (the anterior branches of C1-C4) contains sensory and motor fibers and it controls the motion of the skeletal muscles[15]. In DTC surgery, we used the preserved deep or superficial branches of the cervical plexus which had the appropriate diameter and length to reinnervate the invaded or injured unilateral recurrent laryngeal nerve. Of the 18 cases, there were 15 (83.3%, 15/18) with either entirely or partially restored vocal cord abductional movement after surgery. Throughout the examination by laryngofiberscopy, we found that 1 patient had voice improvement without the paralyzed vocal cord regaining abductional movement; we therefore thought that this could be ascribed to compensation by the contralateral normal vocal cord.
Our data showed that the paralyzed vocal cord was mostly restored after cervical plexus-RLN reinnervation (Figs. 3, 4). The data support the usefulness of cervical plexus-RLN reinnervation for the treatment of unilateral vocal cord paralysis. In this operation, we used 2 different branches of the cervical plexus for the reinnervation. From our data (Table 1), we were able to find that the recovery rate of laryngeal motor function using the deep branch of cervical plexus was better than using the superficial branch of the cervical plexus; however, there were no statistically significant differences between these 2 groups of the patients (P = 0.1). The data also showed that a patients with a history of hoarseness before surgery of less than 3 months (92.3%, 12/13) and of more than 3 months (60 %, 3/5) have a different restoration rate of vocal cord function, and that the effect of reinnervation correlated with the duration of reported hoarseness.

The paralyzed vocal cord before reinnervation.

The abductory motion of the vocal cord restored after surgery.
Crumley[10,11] proposed several possible advantages of laryngeal reinnervation with the ansa cervicalis. i) It had the possibility of resulting in normal or near normal voice without synthetic or anaplastic materials being placed inside the laryngeal framework; ii) it did not alter the stiffness of the vocal cords; iii) it restored bulk to the vocalis muscle; iv) it was reversible; v) it did not preclude static methods if failure ensued; vi) it eliminated dysphonia due to synkinesis if present (by sectioning the RLN). Cervical plexus-RLN reinnervation offers the same advantages as those methods described above, perhaps to a greater extent than ansa cervicalis-RLN reinnervation. This procedure is more convenient during surgery as the donor nerve is located within the surgical field of the thyroidectomy; therefore, the reinnervation can be done simultaneously. The most important advantage of the cervical plexus-RLN reinnervation procedure is that the length and diameter of the donor nerve can be correctly selected during surgery. The ideal surgical procedure is surely the one that provides appropriate resection of the vocal cord mass and adequate tension during phonation, without interference from uncoordinated movements. This technique appears to achieve these goals.
Nerve transfer is still assumed priority in our clinical practice if the operative scenario provides iatrogenic severance of the RLN and if immediate nerve repair is recommended as the primary operation. Otherwise, we perform the nerve implantation as the secondary corrective operation if the patient meets the appropriate criteria, including a laterally paralyzed vocal cord with a mobile cricoarytenoid joint, RLN injury stump found intraoperatively, and a donor nerve free of invasion by tumor, which is the most important criterion.
In a word, cervical plexus-RLN reinnervation is a simple and efficient alternative to nerve implantation. The patients are highly satisfied with this procedure, and reconstitution of the vocal cord may be reliably anticipated.
The surgical techniques of cervical plexus-RLN reinnervation
The effect of cervical plexus-RLN reinnervation relies on the types of injuries to the recurrent laryngeal nerve and the application of a normative surgical procedure, but the surgical techniques are important for the success of reinnervation. Because of the “recurrent” character of the RLN, the central and peripheral part of the graft nerve should not be mixed up with the proximal and the distant part of RLN in reinnervation. Excess nerve should be trimmed in length before anastomosis and the graft nerve diameter may be equal to or slightly larger than that of the stump RLN. Meanwhile, nerve nutritional medicines such as neurotrophic factors used postoperatively help the recovery of the paralyzed vocal cord.
Conclusion
Cervical plexus-RLN reinnervation can reinnervate injured or infiltrated unilateral recurrent laryngeal nerves, as demonstrated in the 18 patients in our study, and functionally where most patients’ paralyzed vocal cords were restored. The cervical plexus-RLN reinnervation procedure could offer a number of advantages over other methods of repairing unilateral vocal cord paralysis and could be the technique that most surgeons choose when treating unilateral vocal cord paralysis. Given this small patient sample, we could not provide a uniform conclusion or an outcome guideline. But we believe that this technique may present surgeons with another tool in the arena of vocal reparation after unilateral vocal cord paralysis. Future studies of this technique used for the patients with RLN with invasion or injury need to be conducted in order to accumulate more experience and to further validate these results.
- Received July 14, 2009.
- Accepted September 17, 2009.
- Copyright © 2009 by Tianjin Medical University Cancer Institute & Hospital and Springer
In this issue






{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.