

Abstract
OBJECTIVE To investigate the clinical effects of the application of double points cryoablation through percutaneous puncture for advanced lung cancer patients.
METHODS Forty-one patients diagnosed with stage III-IV pulmonary carcinoma were selected for the study. The patients were found to have from 1 to 3 foci of carcinoma, and in each case the disease was limited to one lung. The study patients were divided randomly into 3 groups. There were 16 cases receiving routine chemotherapy and radiotherapy in group I, 13 cases treated with cryoablation at a single point in group II, and 12 cases treated with cryoablation at 2 points simultaneously in group III. The patients in the 2 cryoablation groups also received the same treatment as the patients did in group I. The clinical effects were evaluated within 6 months aft er treatment, and the survival rate was followed-up for 3 years.
RESULTS The clinical effects were improved significantly aft er treatment in group II and in group III compared with those in group I (P < 0.05), including an enhanced regressive rate of 21%, postponed tumor progression of 50.58% and a clinical benefit rate of 92%. The effective rate of regression in group III was higher than that in group II, 43.59% (P < 0.05), and the 3-year survival rate was 37.25%. Significant differences in side effects were not found between the 2 cryoablation groups.
CONCLUSION Cryosurgery ablation at 2 points, simultaneously, and directed at 1 foci might improve the effects of treatment and the prognosis of lung cancer patients, when used in combination with routine treatment.
keywords
Introduction
For pulmonary carcinoma patients the taboo treatment modalities of pneumonectomy, chemotherapy and radiotherapy are typically implemented[1-3]. Ablation surgery is a method to utilize energy which is locally released in order to destroy tissue, and the method is becoming an effective local treatment option for malignances which, at present, are usually treated by palliative surgery[4]. Cryoablation has been often used for the treatment of hepatocellular carcinoma, according to the data. Reports in the literature regarding cryoablation for the treatment of lung cancer are sparse[5-7]. Moreover, on a regular basis, foci of carcinoma with maximum diameters of approximately 3 cm-5 cm are treated with single point cryoablation[8]. According to the theory of tumor neovasculature, cytokines secreted from the malignant and normal tissue surrounding a tumor stimulate the proliferation of endothelial cells of small vessels in the normal tissue, forming a new vascular system for the tumor[9]. Tumor vessels are usually distributed densely in the periphery of the tumor. Therefore, double point cryoablation might destroy more tumor cells via the neovasculature. We recently found that within 3 years cryosurgery ablation through double points simultaneously, combined with conventional methods of chemotherapy and radiotherapy, can improve clinical effects for advanced pulmonary carcinoma. Compared with the routinely used single point cryoablation, double point cryosurgery ablation has demonstrated a more significant clinical effect.
Materials and Methods
Clinical data
Forty-one patients in our hospital were diagnosed with pulmonary carcinoma after histopathologic examination during 2000-2004. The clinical stage of each patient was determined through computed tomography. In the 41 cases, there were 27 males and 14 females, with an average age of 54 ± 3.8, ranging from 33-73 year old. The clinical stages of the patients were from stage IIIa to stage IV. The histologic type of the patients’ malignancies was as follows: squamous cell carcinoma in 18 cases, adenocarcinoma in 20 and small cell anaplastic carcinoma in 3. These patients were found having 1-3 foci limited to the lung on one side in each case, and the study patients were divided randomly into 3 groups. In group I, 16 cases were given routine chemotherapy and radiotherapy, in group II, 13 cases were treated with cryoablation at a single point, and in group III, 12 cases were treated with cryoablation at 2 points simultaneously at one focus. The diameters of the foci were 3 cm-5 cm. The regimen of chemotherapy and radiotherapy in the 3 groups were similar. Some of the patients received branchial arteriography and pneumoangiography by which chemotherapeutic agents were administered through the bronchial artery.
Preparing for cryoablation
Before treatment, the patients received routine examination and laboratory studies including those assessing blood cell counts, and hepatic and renal function, as well as electrocardiography, pulmonary function, prothrombin time, and activated partial thromboplastin time. For inclusion in the study, the results of these studies were required to be within normal limits, and the patient’s physical quality grade at/above 60 cents (Kanofsky grade). Those patients with abnormal findings, such as, cardiopulmonary functional defects, emphysema and a tendency for significant hemorrhage, were excluded.
Treatment procedure
Patients received cryoablation after 2 cycles of chemotherapy. Radiotherapy and chemotherapy were applied in sequence after the ablation was completed. The percutaneous puncture point was determined using computed tomography. The diameter of the tumor focus to which the 2 cryosurgery knifes were applied was 3 cm-5 cm or greater, and the distance between the 2 puncture points was 3 cm-5 cm. The distal end of the cryosurgery probe was inserted into the site 1 cm away from the tumor margin. Cooling was performed at a temperature between -125°C – -150°C for 15 min followed by rewarming at 15°C-20° C. The cooling was implemented for 2 cycles. Computed tomographic examination of the thorax was completed as soon as the cryoablation was finished. If a pneumatothorax occurred, thoracentesis was used to remove the air in the thoracic cavity.
Post-cryoablation management
After cryoablation, antibiotics and hemostatic agents were administered and vital signs such as blood pressure, pulse, respiration and saturation of blood oxygen were monitored routinely utilizing an electrocardiogram. Chest X-rays were taken routinely 3-5 days after cryoablation. Thoracentesis or closed drainage of the thoracic cavity was administrated as soon as pneumothorax or hydropneumothorax was diagnosed.
Observed markers
All cases were observed along with chest X-rays, and when foci appeared to decrease in size, computed tomography was implemented to record the change. Chest roentgenograms were checked up to once a month for 4-6 months. CT was taken at the end of last cycle of chemotherapy. The clinical effect was evaluated according to the estimated standard of clinical treatment effect on solid tumor of WHO (complete regression, partial regression, stabilization and progression). Patients with elevated serum carcinoemnryonic antigen had neuron specific enolase, Ca199, Ca153, Ca125 checked monthly for 12 months. The survival rate was investigated for 3 years.
Equipment of cryosurgery ablation
The Endocare Cyrocare System is a device which induces cryosurgery ablation with argon and helium air and is produced by Endocare Co. USA.
Statistical analysis
Data were analyzed with professional statistical software, SPSS 10.0. Enumeration data were statistically evaluated using the rank sum test and the Chi-square test, while measurement data were analyzed with the student t test, α = 0.05.
Results
Rates of tumor regression
Tumor regression was not distinct within 3 weeks after cryosurgery. Bloody phlegm was present 2 or 4 days following surgery and continued usually for 1-2 weeks. The phlegmatic secretions were occasionally dark violetred in color due to the presence of necrotic tissue. After routine radiotherapy and chemotherapy, shrunken foci or even central cavitation was seen. The patients who received chemotherapy or radiotherapy still obtained significant clinical effect after local treatment. One case of small cell pulmonary carcinoma could not be treated with chemotherapy because the cellular toxic agents induced damage to renal function and elevation of serum creatinine up to 2 times more than normal limits. The malignant foci remained in partial regression and stable for 2 years after receiving cryosurgery ablation. According to measured results from computed tomography, the treatment effect of patients in the groups undergoing cryoablation with routine therapy (group II + III) were better than those in the routine therapy group, as indicated by the number of cases showing partial regression, progression and tumor progression (Table 1). Compared with group I, the clinical effects in groups II and III were improved significantly including an increased regression rate of 21%, a rate of postponement of tumor progression of 50.58% and a clinical benefit rate of 92% (P < 0.05). Several clinical markers showed that the rates of clinical effectiveness in the patients treated by double point cryoablation were better than those of the patients treated by single point cryoablation in (Table 2). The effective regression rate of the patients treated with 2-point cryosurgery increased to 43.59% compared with that of the patients treated with single point cryoablation (P < 0.05). Focal liquefaction of the malignancy in the patients in group II was more significant than that in group III. Therefore, the effects in group III were more marked due to the cavitation of the foci 6 months after cryoablation (Figs. 1, 2). In addition, bronchial arteriography or pneumoangiogram offered reference for selection of the puncture site in some of the patients who received chemotherapy delivered through the bronchial artery (Fig. 3).
Effects of cryosurgery ablation on pulmonary carcinoma.
Comparison of clinical effect between the 2 groups with cryoablation.
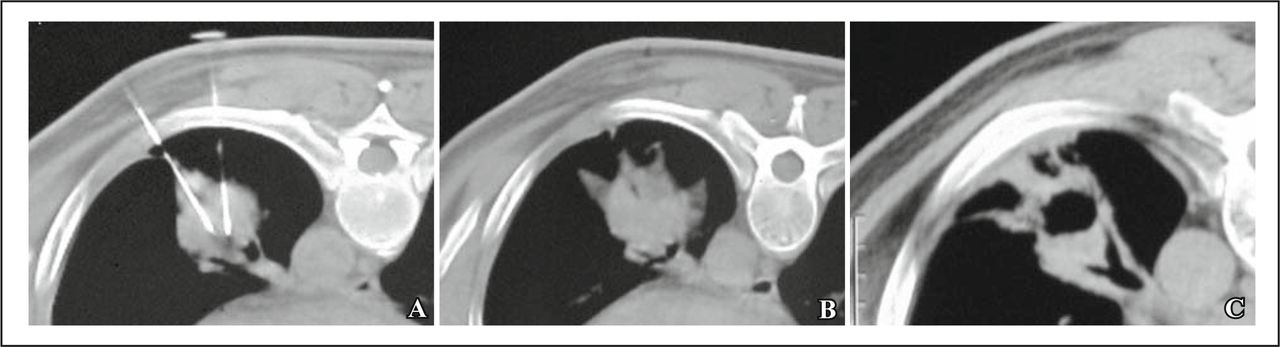
(A): Before cryoablation, double point puncture was performed on a malignant focus of the left lung, guided by computed tomography. (B): The altered focus in left lung received cryoablation at the end of treatment. (C): A thin-walled cavity formed in center of the foci after cryoablation combined with chemotherapy and radiotherapy.
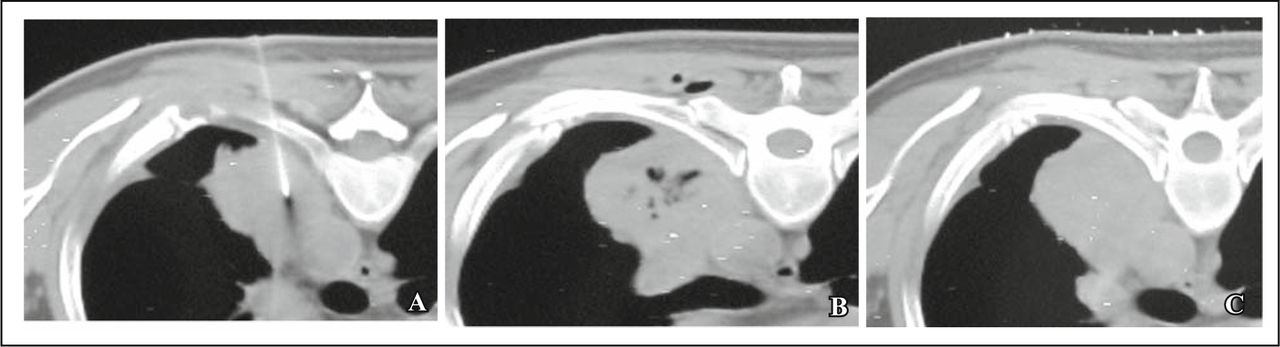
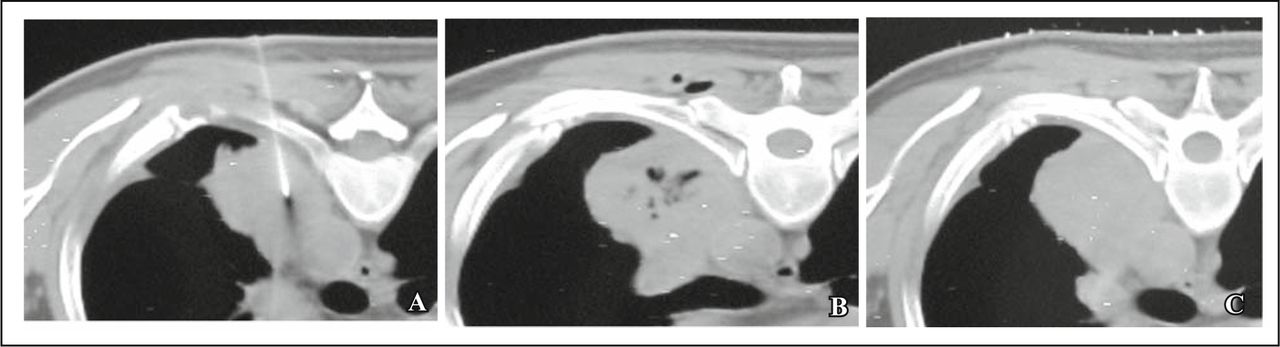
(A): Before cryoablation, single point puncture was performed on a malignant focus of the left lung, guided by computed tomography. (B): The altered focus in the left lung received cryoablation with small regions liquefaction formings at the end of the treatment. (C): The foci of pulmonary cancer did not have obvious changes after cryoablation combined with chemotherapy and radiotherapy.
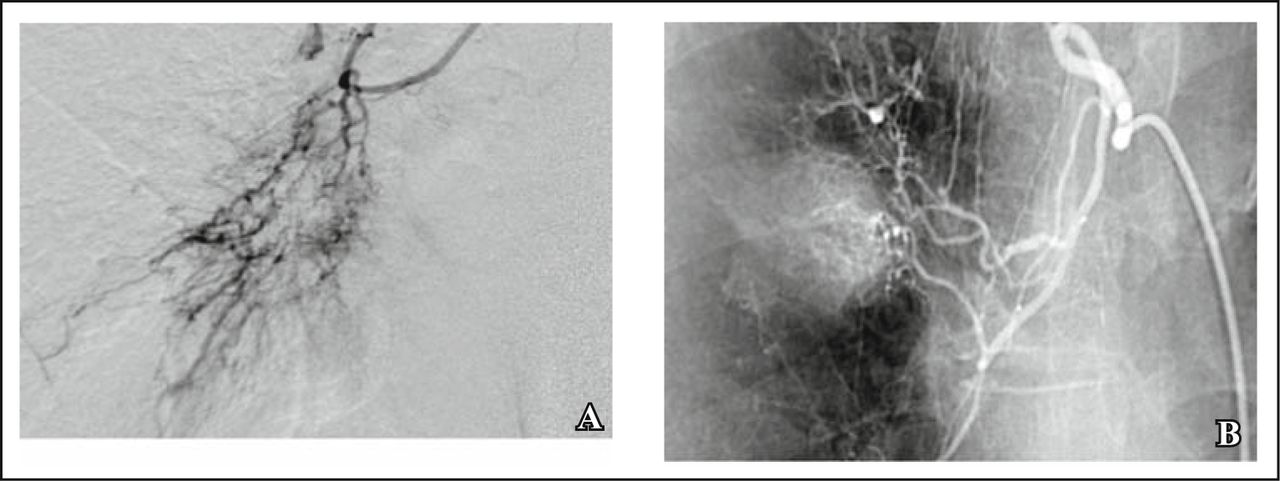
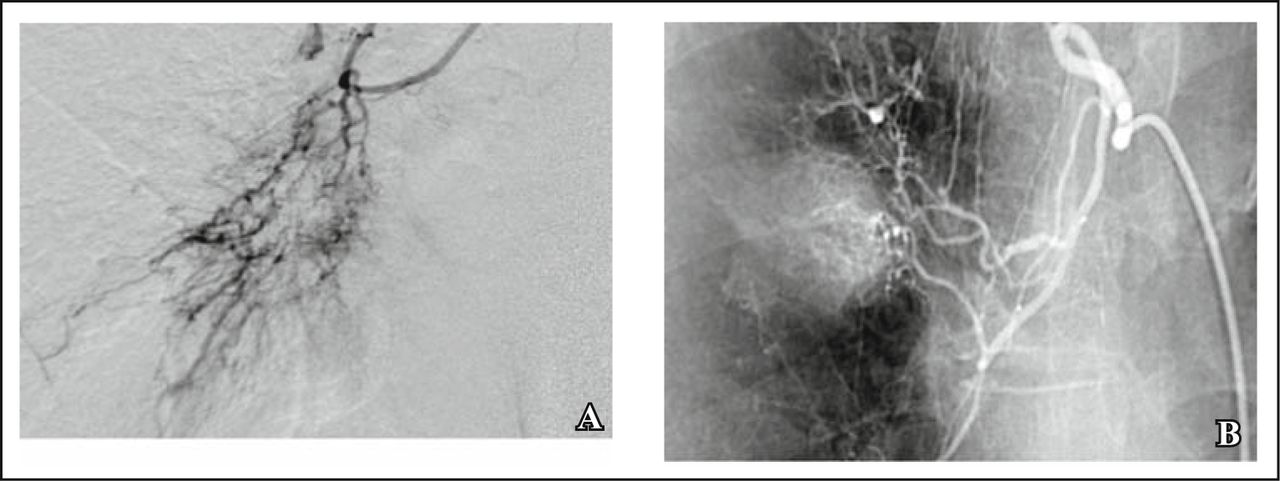
Bronchial arteriography and pneumoangiogram before cryoablation (A&B).
Serum carcinoma markers
The patients in group II and group III presented with decreased levels of several serum tumor makers, and the rate of decrease in these patients was 52% (13/25), in markers such as carcinoemnryonic antigen, neuron specific enolase, Ca199, Ca153, Ca125. However, statistically significant differences were not found in the tumor markers among the 3 groups.
Survival rate
The 3-year survival rate in group I was also improved (3/16, 18.75%, routine therapy group) compared with that in group II and group III (14/25, 56.0%, cryoablation groups), i.e. 37.25%.
Side effects of cryosurgery ablation
The patients in group II and group III all received local cryosurgery by way of percutaneous puncture. The side effects of local cryosurgery included pain around the sites of puncture and absorption fever lasting for a short time. Bloody phlegm occurred at the rate of 32.0% (8/25), 3 cases in group II and 5 cases in group III (P > 0.05). Pneumothorax occurred at a rate of 25% (5/25): 2 cases in group II and 3 cases in group III (P > 0.05). Small pleural effusions were present, producing blunting of the costophrenic angle on chest roentgenograms, but large effusions developed in a few cases, 28.0% (7/25), 3 cases in group II and 4 cases in group III (P > 0.05). Encapsulated effusions occurred around the site of puncture in 2 cases.
Discussion
Regarding therapy for pulmonary carcinoma, surgery is typically selected first, and is followed by adjuvant chemotherapy and radiotherapy. This therapeutic regimen adapts to most patients with pulmonary cancer in stage I-IIIa. However, some patients cannot receive this regimen such as those with central pulmonary cancer, those with metastases to mediastinal lymph nodes or to the opposite lung and those with other complications. Therefore, alternate modes of treatment for these patients should be offered for the same purpose of effectively controlling tumor progression and shrinking malignant foci. Treatment by tumor ablation is a type of method which includes radiofrequency and microwave thermoablation therapy as well as the more recently developed cryosurgery ablation which was introduced at the beginning of this century[10-12]. These measures of ablation have been used for treating several neoplasms including lung carcinoma[13,14].
The function of cryosurgery ablation in cancer treatment is mainly to destroy the malignant tissue and cells. A curative outcome may occur if the region of cryoablation entirely envelops the malignant tissue. The “cryoablation region” is usually a regular ellipse[8,11], whereas the shape of a malignant tumor is frequently anomalistic. Therefore, the “ablation region” infrequently surrounds a tumor completely. As a result, other methods of local treatment still need to be utilized for further therapy so as to improve clinical effect[8]. One of the rules in treating carcinoma is integrating local treatment with whole body therapy for enhancement of clinical effect. Therefore, this study has shown that the combination of cryotherapy with chemotherapy and radiotherapy improved clinical outcome effectively. Namely, partial regression was seen in some cases, stable foci occurred in most cases and the time to tumor progression was modified as well. Further, prognosis was ameliorated compared with patients treated by routine therapy.
The doctrine of new tumor angiogenesis suggests that the root of tumor neovasculature is in the normal tissue which surrounds a malignant tumor[9]. Cancer cells usually proliferate actively in regions of blood vessel exuberance which are in close proximity to neoplastic tissue. Cell multiplication is usually more inactive in regions where blood vessels are sparse, typically in the central regions of malignant neoplams; spontaneous necrosis can occur here as well. Several cytokines secreted from tissues of malignancies and hosts are primary factors in stimulating the formation of tumor neovasculature. Interdiction of the blood supply to tumors may promote inhibition of the proliferation of malignant cells. This theory has been driving research and the development of treatments directed against malignant vasculature[15-18]. Based on this theory, we have observed, through by bronchial arteriography or pneumoangiography, that the vessels of pulmonary cancer in the vessels of normal lung are similar to a “bird’s nest” inhabiting a branch of tree. These findings also suggest that tumor vessels begin from the vascular system of host tissue. Moreover, an intensive region of tumor vessel growth is localized to the peripheral part of carcinomas while sparse regions of vessel proliferation are localized centrally. The central region of a tumor is typically used as the area for puncture in a majority of ablations. In this way, the center of the ablation region is usually at the central part of tumor, and the ablation is relatively weak in the region of intensive vasculature and active proliferation of cancer cells. However, double point cryosurgery ablation is ideal in obliterating the intensive region of vessel growth and in destroying the blood supply of carcinomas when the region of active multiplication is ablated. The effects to the malignant tissue can be drastic. The results of this study suggest that single point cryoablation can produce a more obvious effect within a small region, but its long-term effect is not as good as those of double point cryosurgery ablation.
The diameter of the cryoablation probe is 3 mm, and its active extent is about 30-50 mm in diameter[7]. However, our probe, when applied in practice, showed that the treatment effect with single cryoablation was not as obvious as that with double point cryosurgery ablation. The reasons may involve 3 presumptions. First, the “thermo-pool effect” might weaken the action of single point cryoablation, namely the blood supply around the tissue, which would decrease the extent of the cryocare function[19]. Second, the active part of single point cryoablation is at the center of the neoplasm. The vascularity in the center is less than that in circumferential part of the tumor, and thus, cryoablation does not destroy the blood supply of tumors and the active region of proliferation of cancer cells, which can lead to recurrence[16,17]. Third, normal tissue surrounding a tumor might be also damaged to some extent due to extending the cryoablation area, and cellular function could be affected in this surrounding normal tissue. The effect would involve secretion of cytokines stimulating angiogenesis and inhibiting hyperplasia of the neovasculature. These are the conjectures coming from tumor neovasculature theory directed towards improving the clinical effects of treatment with double point cryoablation. Further research is need for confirmation.
In conclusion, cryoablation combined with routine therapy might improve the clinical outcome for pulmonary carcinoma patients. Double point cryoablation, in comparison to the more commonly used single point cryoablation, could offer a better prognosis for patients with lung cancer.
- Received May 9, 2009.
- Accepted October 9, 2009.
- Copyright © 2009 by Tianjin Medical University Cancer Institute & Hospital and Springer
References
In this issue






{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.