

Abstract
OBJECTIVE To analyze and discuss about the clinical characteristics, pathological types, surgical modalities and techniques, and postoperative complications in children with tumor of posterior cranial fossa.
METHODS Retrospective study was conducted on 102 cases of pediatric tumor of posterior cranial fossa, admitted and treated in our hospital during the period of January 1996 to January 2007. All patients underwent microscopic surgical treatment. Fifty-eight were male and 44 cases were female. The age ranged from 9 months to 14 years old, with an average of 6.1 ± 0.5 of age. Cranial CT or MRI examination was conducted before and after the surgery on all patients.
RESULTS The primary manifestations for this group of patients were increased intracranial pressure and/or ataxia. Postoperative pathological diagnoses showed: 46 cases of medulloblastoma, 43 cases of astrocytoma, 11 cases of ependymoma (including 1 case of degenerative ependymoma), 1 case of dermoid cyst, and 1 case of teratoma. In this group of the patients, radical surgery was used in 68 cases and subtotal surgical removal used in 31 cases, while surgical removal of large section was performed on 3 cases. There were no deaths from surgery reported. Ninety-one cases showed significant symptomatic improvement when compared with preoperative conditions, while 11 cases showed either no improvement or more severely affected afterward. For 6 cases, postoperative ventriculoperitoneal shunt was performed within 7 days to 2 months after the surgery. Sixty-three patients gained follow-up for 3 to 60 months in duration. Thirty-nine patients regained normal life and were able to learn well, while there were 7 patients who could not live normally on their own. During the follow-up period, there were 17 cases of recurrence and 7 cases of death. In 23 cases of medulloblastoma in children with age of 3 years old or above, 2 cases who underwent surgical removal of intracranial ependymoma received small dosage of postoperative X-ray radiotherapy on the the brain and spinal cord. Nine cases of medulloblastoma in children under age of 3 and 17 cases of astrocytoma diagnosed after the surgery received chemotherapy of Carmustine.
CONCLUSION Medulloblastomas and astrocytomas were the most common types of pediatric tumor of posterior cranial fossa, right followed by ependymoma, and dermoid cysts and teratomas were rare. Early correct diagnosis, proper selection of appropriate surgical modality and the surgical margin, proper treatment of postoperative complications, and the selecting right radiotherapy or chemotherapy were the key factors in influencing the prognostic outcome of children with tumor of posterior cranial fossa.
keywords
Introduction
Pediatric tumor of posterior cranial fossa accounts for 60% to 70% of intracranial tumor seen in children[1]. The clinical manifestations of pediatric tumor of posterior cranial fossa appear late and the tumor tends to be large in size. Because its location is deep and closely related to the surrounding brain stem, important peripheral nerves, and blood vessels, its radical surgical removal is fairly risky. The questions of how to improve the accurate rate of diagnoses and the effective rate of surgical removal, how to avoid the occurrence of severe complications, are extremely important for the prognostic outcome for the patients. And these are the challenges that neurosurgeons face. Our hospital admitted and treated 102 cases of pediatric tumor of posterior cranial fossa during the period of January 1996 to January 2007. Now, a retrospective analysis was conducted to investigate its clinical manifestations, diagnostic examinations, pathological characteristics, surgical modalities and techniques, and the treatment for postoperative complications. This study will hopefully provide information to improve the therapeutic effect when treat the children with such tumors.
Materials and Methods
General information
In this group of 102 patients, 58 were male and 42 were female. The age range was from 9 months to 14 years old (average of 6.1 ± 0.5), 21 of them under the age of 3. Thirty-eight patients were between 4 to 7 years old, 30 patients between 8 to 10 years and 13 patients between 11 to 14 years old. Clinical course was around 3 weeks to 1 year, with an average of 4.5 months.
Clinical presentations
The primary manifestations for this group of patients had increased intracranial pressure and/or ataxia, in which 74 cases had increased intracranial pressure and 41 cases with ataxia. Eight patients showed symptoms of involvements in cranial nerves of posterior group and neurone in the brain stem. Five patients complained of diplopia or showed paralysis in extraocular muscles. Four cases had forced head position and 2 cases suffered epileptic onset.
Image examinations
Regular scanning or enhanced scanning of head CT or MRI was performed for all patients. Images showed that 27 cases located in the cerebellar hemisphere, 51 cases located in cerebellar vermis and 24 cases located in the fourth ventricle. Sixty cases had diameters ranging from 2.5 cm to 4 cm, while 42 cases showed size of tumor larger than 4 cm. Thirty-seven cases had different degree of supracerebellar hydrocephalus and 21 cases showed tumor with cystic lesion.
Therapy modalities
All patients received surgical removal of tumor under microscope. The ventriculoperitoneal shunt was performed on 3 patients 7 days before the surgery. The ventriculopuncture drainage was performed on 5 patients 1 to 3 days before the surgery. The best surgical approach was selected according to the location of tumor. Sixty-seven cases received the approach of supraoccipital medium route and 35 cases had the approach of supraoccipital para-medium route. In 40 cases, the cut was made below the occipital region of posterior cranial fossa, while the bone flap was removed as well. Sixty-two cases were given the craniotomy. Y-shaped or H-shaped cut was used for the incision at epidural region. For infants, the epidural incision must be carefully made to mind the occipital sinus and the atlas sinus because their immaturity could cause acute bleeding and even the danger of ischemic shock. In the surgery for tumor in the fourth ventricle, it must be noted to relieve the obstruction of aqueduct in midbrain and the CSF circulation pathway must be re-established. The epidural suturing must be tightly made after the removal of tumor and the missing part must be fixed and covered with biological protein gel. For some cases with medulloblastoma and ependymoma (25 cases), postoperative radiotherapy must be performed. Some patients with astrocytoma (17 cases) underwent postoperative chemotherapy with Carmustine.
Results
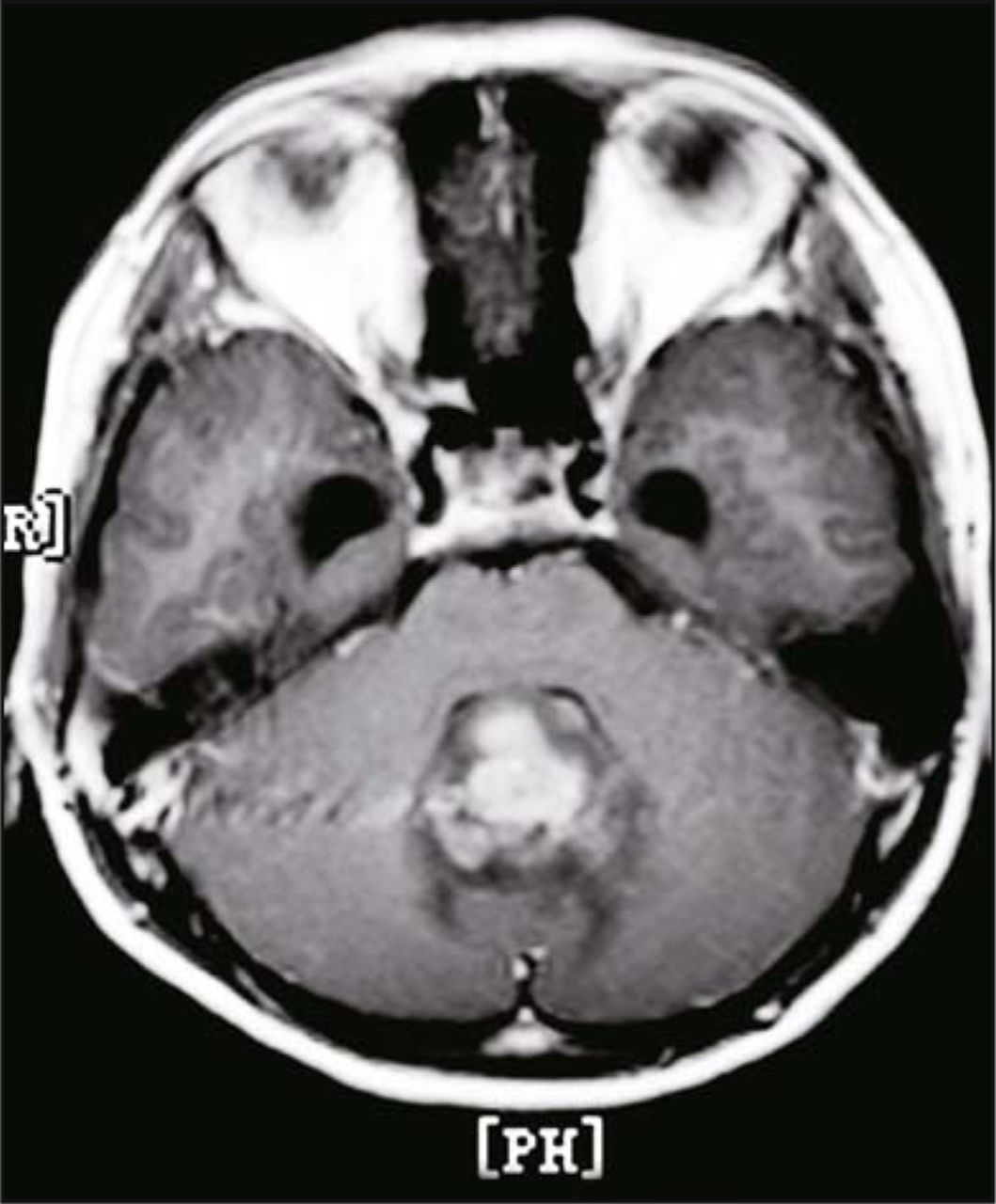
Postoperative pathological diagnoses of 102 cases showed: 46 cases of medulloblastoma, as shown in Fig. 1, 43 cases of astrocytoma, 11 cases of ependymoma (including 1 case of degenerative ependymoma), 1 case of dermoid cyst, and 1 case of teratoma, as shown in Fig. 2. In this group of patients, complete surgical removal of tumor was performed on 68 patients (66.7%) (including 23 cases of medulloblastoma, 35 cases of astrocytoma, 8 cases of ependymoma, 1 case of dermoid cyst, and 1 case of teratoma). There were 31 cases that underwent subtotal incision (30.4%) (including 23 cases of medulloblastoma, 6 cases of astrocytoma, 1 case of ependymoma, and 1 case of degenerative ependymoma). The surgical removal of large section was performed on 3 cases (2.9%) (including 2 cases of astrocytoma and 1 case of ependymoma). There were 91 patients whose symptoms were improved significantly, 7 patients whose symptoms were not significantly improved after the surgery, and 4 patients whose symptoms were aggravated. Secondary cerebellar hematoma occured in 1 case and the gas accumulation in ventricle happened in 4 cases. Postoperative complication such as mutism was presented in 2 patients, but they recovered within 1 to 2 months after the surgery. Postoperative liquid accumulation in residual cavity and non-bacterial meningitis were seen in 5 patients, and they also recovered after conservative treatment. The ventriculoperitoneal shunt was performed on 6 patients 7 days to 2 months after the surgery. There was no perioperative death reported.

Male, 3-year-old, Preoperative axial MRI showed tumor located at the central part of cerebellar vermis. Tumor grew into the fourth ventricle, and the size was approximately 4 cm × 4.5 cm. The signal was uneven, and the enhancement scan showed stronger uneven signal. There was sign of obstructive hydrocephalus. Postoperative pathological diagnose showed medulloblastoma.

Female, 4-year-old, Preoperative MRI showed tumor located at the central part of cerebellar vermis. Tumor pressed the fourth ventricle, and the size was approximately 4 cm × 5 cm. The enhancement scan showed stronger even signal. There was sign of obstructive hydrocephalus. Postoperative pathological diagnose showed teratoma.
Twenty-three cases of medulloblastoma at the age around 3 (11 cases of radical resection, 11 cases of subtotal resection, and 1 case of surgical removal of large section) and 2 cases of ependymoma (one case for each: radical and subtotal surgery) received low dosage of X-ray radiotherapy on the nerve axons of entire brain and spinal cord. The radiotherapeutic proposal and dosage were individualized by professional radiologist according to the patient’s conditions. For patients who received radical resection of ependymoma and astrocytoma, they did not receive further radiotherapy. Nine cases of medulloblastoma in children under the age of 3 and 17 cases of postoperatively diagnosed as astrocytoma received chemotherapy with Carmustine for 3 days each time and 3 times for the first year. Any additional treatment would be based on re-imaging examination and individual conditions.
Sixty-three patients received follow-up with duration of 3 to 60 months. Thirty-nine patients returned to normal life and were able to learn well. Seven patients lost the ability to take care of themselves. During the follow-up period, there were 17 who recurred (4 with radical removal of medulloblastoma, 7 with subtotal resection, 1 with radical resection of astrocytoma, 3 with subtotal removal, and 1 with both subtotal and radical removal of degenerative ependymoma in different times). Seven patients died during the follow-up period.
Discussion
The tumor of posterior cranial fossa is more common in children than in adults and takes about 60% to 70% of noted pediatric intracranial tumors. The most common pathological types of pediatric tumor of posterior cranial fossa were medulloblastoma and astrocytoma right followed by the ependymoma[1-3]. The statistical analysis in this study showed that the order of the onset for the first three places were medulloblastoma, astrocytoma, and ependymoma, and accounted for 45.1%, 42.2%, and 10.8%, respectively.
The diagnosis of pediatric tumor of posterior cranial fossa primarily relies on clinical manifestations and image examination. Clinical manifestations vary from person to person and the tumor is commonly seen near the center location of posterior cranial fossa. In addition, children are growing and developing, and thus, their clinical manifestations lack specificity and accuracy in description. Early manifestations due to an injury in the nervous system are usually ignored, and the tumor has already become large in size when diagnosed. Increased intracranial pressure is most commonly seen as an early symptom. It was found in up to 72.5% of our studied group of patients. When the tumor grows and blocks the aqueduct of midbrain, it causes the obstruction in the circulation of CSF. The ventricular system expands resulting in the symptoms of increased intracranial pressure such as headache, vomiting, and papilloedema. Infants, on the other hand, show venous engorgement in the scalp and become irritable with constant vomiting. These are commonly misdiagnosed as digestive disease, causing delay in proper treatment. In this group of patients, 2 cases showed only intermittent vomiting at the beginning and had a few months of treatment based on being misdiagnosed as dyspeptic stomach before diagnosed as the tumor of posterior cranial fossa by head CT examination. It deserves more attention from researchers. Also, the cerebellar symptoms include bodily ataxia such as imbalanced walking. This symptom occurred in 40.2% of children studied. Some patients showed manifestations of involved cranial nerves of posterior group and neurone of brain stem, such as vomiting, hiccup, bucking, hoarseness, and etc., which comprised 7.8% of studied patients. Some patients only came to hospital because of the paralysis in extraocular muscles. Diagnosis based on image examination requires imaging characteristics of different tumors and needs a comprehensive judgment along with onset age and onset location in children.
Surgical treatment is the primary method for treating pediatric tumor of posterior cranial fossa. The principle of surgery is to ensure the maximum removal of tumor mass under the circumstances of protecting brainstem from injury, while opening up the circulation of CSF. Most medulloblastoma originate from the cerebellar vermis and have clearly definite margin separated from soft texture. The approach of surgical removal of tunnel style is usually taken. Usually, it does not adhere to the fourth ventricle, but it is only separated from the cerebellar tissues with an interface in between because medulloblastoma has no enclosing membrane. During the process of surgical removal, this interface must be kept clear, or else, residual tumor mass may adhere to it and cause a recurrence. In this group, the complete resection rate of medulloblastoma reached 50.0% (23/46). Postoperative recurrence is not only related to the degree of severity of the malignant tumor, but also related to unintended residues of tumor mass. Astrocytoma, which is mostly low malignancy, originates from cerebellar hemisphere and cystic degeneration is usually seen. Complete resection is also recommended and the removal of tumor nodules is a must during the surgery. Few astrocytomas also originate from the brainstem. The complete resection rate is related to the extent of involvement of the brainstem. In this study, the complete resection rate was 81.2% (35/43). The 8 cases that underwent subtotal resection and partial resection had the tumor originated from brainstem and had the symptoms induced from the brainstem involvement.
Ependymoma is different from astrocytoma in which the ependymoma grows in an expansive pattern, while the latter one shows an infiltrative growing pattern. Tumor usually shows a clear and definite borderline with the surrounding normal tissues and complete resection can cure the disease[4]. Therefore, the complete resection must be performed if at all possible. But because it mostly originates from the bulbar region of the fourth ventricle and involves severe adhesion to the surroundings, the complete resection is difficult But it is especially difficult when the tumor grows on one side, such as when it grows on the side of pons and cerebellum that involves facial/auditory nerves, trigeminal nerve, and the important crossing branch of anteroinfereior cerebellar artery and basal artery. This is why partial resection is performed. From our experience, it is suggested that it is better to perform partial resection of tumor in the fourth ventricle, to provide adequate space for the next step that involves the resection of cerebellar peduncle and tumor of CPA. The intensity of electrocoagulation must be appropriately adjusted to avoid thermal damage. Sometimes, the tumor mass has to be left to avoid injury to the brain stem. In this study, the complete resection rate of ependymoma was 72.7% (8/11).
Most children of pediatric tumor of posterior cranial fossa have obstructive hydrocephalus before the surgery and have the risks of causing acute high cranial pressure and brain hernia. When it is necessary, ventriculoperitoneal shunt or ventriculopuncture drainage is performed before the surgery, even though they may develop intracranial infection and obstructive shunt [5,6]. In this study, 5 patients received ventriculopuncture drainage 1 to 3 days before the surgery, while 3 patients received ventriculoperitoneal shunt 7 days before the surgery. We believed that children with worsening acute high cranial pressure could undergo ventriculopuncture drainage 1 to 7 days before the surgery. This would allow more time for surgery and more relief from intracranial pressure because of the surgery which minimizes the possibility of hydrocephalus. For patients who cannot receive surgical removal of tumor mass within 7 days after having the ventriculopuncture drainage, ventriculoperitoneal shunt should be performed to provide better surgical conditions and avoid the possible intracranial infection due to long-term ventriculopuncture drainage. The surgery should be given as early as possible. For most patients where there is not a serious condition of acute high cranial pressure, the CSF can be slowly released from the cut at the occipital pool during the surgery. When it is necessary, temporary puncture at posterior ventricular peduncle allows a temporary relief from high pressure. The most commonly seen postoperative complication in children with tumor of posterior cranial fossa is the secondary hydrocephalus which will worsen the condition. The causes are: postoperative edema of cerebellum, obstruction to CSF re-absorption due to subarachnoid hemorrhage, adhesion of the opening to the fourth ventricle and its surroundings, and etc.[7,8] Postoperative hydrocephalus is the most severe complication of the surgery for pediatric tumor of posterior cranial fossa and even endangers life if not properly treated. Therefore, soon after the surgery, ventriculoperitoneal shunt or ventriculostomy under neuroendoscope should be performed if circumstances allow. In this group of patients, 6 underwent postoperative ventriculoperitoneal shunt. The immediate effect is good, but long-term installation has the disadvantages of obstruction and is worrisome to the children and parents. In recent years, with the advancement in minimal invasive neurosurgery, the ventriculostomy under neuroendoscope may become one of the most effective and safe methods in relieving postoperative obstructive hydrocephalus[7]. It still needs further study and practice. Secondly, the secondary intracranial infection after the surgery, which causes refractory fever, is also an important complication. Most cases who develop the infections are due to liquid accumulation in subcutaneous residual cavity at the posterior cranial fossa. The key to prevention is the tight suturing of epidural membrane after the tumor resection. It is important to make sure that the epidural membrane is expanded, and it is fixed and covered with biological protein gel if is necessary in the surgery. In recent years, we performed craniotomy of posterior cranial fossa and initial results showed that this modality not only relieved the psychological burden in children, but also reduced the incidence of refractory fever due to residual liquid accumulation in cavity.
The treatment for pediatric tumor of posterior cranial fossa should include comprehensive perioperative therapies. For malignant pediatric tumor of posterior cranial fossa, treatment relies on complementary radiotherapy and/or chemotherapy on the basis of performing surgery[8]. Debate remains on the question of how to select complementary therapies which are suitable for the certain pathological types of the tumor[8-10]. We believed that therapy should be individualized, according to the age of the patients, the characteristics of tumors, surgical conditions, and tumor’s sensitivity to radiotherapy and chemotherapy. Because radiotherapy has more of effect on children’s nervous system, the low-dosage x-ray radiotherapy on neural axons of the the brain and spinal cord was only performed in 23 patients of medulloblastoma at the age of 3 or above and 2 patients with ependymoma. The patients who received complete resection of ependymoma and astrocytoma did not receive radiotherapy. Nine cases of medulloblastoma at the age under 3 and 17 cases of astrocytoma underwent chemotherapy of Carmustine after surgery. Initial results showed that postoperative chemotherapy and radiotherapy could reduce the recurrence rate. Because of the limitation of sample size in our study, the statistical analysis of larger size of samples with various complementary therapies is still required and will allow us to make further conclusions
- Received November 5, 2008.
- Accepted March 26, 2009.
- Copyright © 2009 by Tianjin Medical University Cancer Institute & Hospital and Springer
In this issue






{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.