

Abstract
OBJECTIVE To explore the value of fiberoptic ductoscopy in diagnosing and treating bilateral and polyporous nipple discharge (ND).
METHODS Fiberoptic ductoscopy was conducted in 29 patients with bilateral and polyporous ND. After the ductoscopy, the patients with intraductal papilloma (IDP) underwent a surgical procedure, and the others, identified with galactostasis, mammary duct ectasia (MDE) and obstructive galactophoritis (OG), received a ductoscopy-guided interventional therapy.
RESULTS Among 29 cases, and with 79 galactophores examined, IDP was found in 11 cases (37.9% of the total cases), or 13.9% of the galactopores examined. IDP was found in 9 of 11 cases with a bloody nipple discharge, while IDP was seen in 2 of the 18 cases with a non-bloody nipple discharge. The excision accuracy achieved 100% in the cases, and postoperative pathological diagnosis accordance rate reached 88.9%.
CONCLUSION Fiberoptic ductoscopy has many features such as ability to see the lesion, and accurate preoperative localization, thus eliminating excessive excision of tissue during surgery. For most patients with ND, especially those suffering galactostasis, OG or MDE, washout under fiberoptic ductoscopy and interventional therapy may achieve a thorough cure of the disease.
keywords
Introduction
Nipple discharge (ND) is one of the presenting symptoms of mammary diseases, accounting for 7.4% of the cases with breast disorders[1]. Except for systematic and medicamentous factors, as well as the possibility of a hypophyseal tumor, most NDs result from intraductal diseases, among which intraductal chronic inflammation, intraductal papillomatosis or duct cancer make up the major proportion[2]. These diseases comprise approximately 2.33%~17.5% of mammary diseases[3]. Introduction of the ultrafine fiberoptic ductoscope (hereinafter designated as a breast ductoscope) has overcome the shortcomings of a polyrrhea smear exfoliocytological examination and selective galactography, which have a low positive rate and poor sensitivity. Presently the breast ductoscope has become an important milestone in diagnosing and treating mammary diseases. The following are the results of our studies on patients with bilateral and multiporous ND who received fiberoptic ductoscopy during a period from March 2006 to September 2007.
Patients and Methods
General data
The ages of our 29 non-lactational female patients were from 23 to 71 years, averaging 44.9 ± 13.0. All patients had bilateral lactiferous duct ND from 2 or more galactophores, with a course of ND ranging from 2 days to 3 years. A total of 79 lactiferous ducts were examined.
Methods
Type of mammary duct treatment
Examination of galactophores with a bloody nipple discharge (BND) is very necessary. For the patients with a mammary lump, the lactiferous duct of the quadrant where the lump was found should be examined, with an one-by-one inspection as far as possible of all the lactiferous ducts producing the ND. As for the patients with a non-bloody nipple discharge (non-BND), and ND from more than 4 galactophores, without a mammary mass, selective examination of each of the galactophores with ND was conducted based on a sequence of upper external, upper inner, lower external, lower inner and central quadrant.
Instruments
Manufactured by the Japan FiberTech Co., the FT-201-type extra-fine and ultra-wide field fiberoptic ductoscope system mainly includes the lactiferous duct dilator, fiberoptic ductoscope, cold light source, displayer, image selector and microcomputer image recording system.
Procedures and collection of data
The patients were instructed to disrobe, and to assume a supine position, allowing a separate examination of each breast. Conventional sterilization of the breasts was conducted, with the nipple being the most important. The open pores of the mammary ducts to be examined were found first, and then a galactophore dilator was used to broaden and distend the galactophores by grades, from small to large (000-07). Approximately 0.2 ml of 2% lidocaine was slowly infused to the ducts at a dilation grade of 01 to provide local anesthesia. The dilation was not ended until a distension by the grade-07 dilator was achieved. The fiberoptic ductoscope was inserted into the dilated lactiferous open pore of the mammary duct, and a 20-ml injection syringe was used to slowly infuse a 0.5%-metronidazole or chymotrypsin solution, distending the occlusive lumens to facilitate the examinations. The galactophorous ducts of grade-I, II and III, or higher grades, and their branches were in turn examined. At the same time, the image was clearly shown on the monitor by signal transmission, and the pictures needed were obtained using a frame selector.
Following the examination, the breasts were massaged along the orientation of the mammary ducts, in order to discharge the perfusate and gas, and to collect the rinse solution for related chemical analysis. The nipples were cleaned again, and coated with mupirocin. After an aseptic dressing was overlaid on the nipples, the patients were told not to bathe for 24 h. Based on the clinical examination a diagnosis was made and a report printed out.
Statistical analysis
In Table 1, IDP occurred in patients with both BND and non-BND. The Chi-square test was used to compare the groups.
The condition of IDP in patients with bloody and non-bloody nipple discharge.
Results
In all of the 11 BND cases with polyrrhea, upon examination of 12 galactophores, BND was found in 1 or 2 galactophores. The nipple discharge from other pores included colorless or yellow and transparent ND, accounting for 37.9% of the cases, and 15.2% of the examined ND galactophores. Among these cases, 6 were big-duct papilloma (BDP) and 1 infitrating ductal carcinoma, all with a postoperative pathological confirmation, and 2 were BDP (including the malignancies), which were confirmed as BDP complicated with a moderate or severe epithelial atypical hyperplasia. Mammary duct ectasia (MDE) and galactophoritis were found in other non-BND mammary ducts.
A 26-year old patient at the end stage of her pregnancy had a polyporous ND, i.e. a bilateral uniforate BND. Ductoscopy demonstrated that it was ductal ectasia complicated with an OG and lactifeous ductal-wall capillary rupture and hemorrhage. The postnatal haemorrhage disappeared following a mammary duct endoscopeguided medicinal rinsing. MDE, complicated with OG, occurred in another case.
Table 1 shows that IDP was found in 11 of the 29 cases, among which haemorrhage occurred in 9, accounting for 81.8% of the BND cases. There were 2 patients with IDP among the 18 non-BND cases, accounting for 11.1% of these cases, resulting in a statistically significant difference between the two groups, P = 0.000246, P < 0.001. Intraductal papilloma occurred in 11 of the 79 mammary ducts examined. BND was seen in 9 (75.0%) of the 12 galactophores. Non-BND cases were found in 2 of the 67 galactophores, accounting for 3.0% of the non-BND ducts. There was a statistically significant difference between the two groups, χ2 = 38.096, P < 0.001.
The accuracy of focal excision was 100%, and the accordance rate of postoperative pathological diagnosis was 88.9%. The intraductal space-occupying lesion cases made up 37.9% of the total cases, and 13.9% of the examined galactophores.
Milky nipple discharge occurred in 4 cases, over a period of 7 days to 2 years. Laboratory examinations showed that the values of all hypophyseal hormones were normal. One case with unilateral uniforate polyrrhea was diagnosed as BDP complicated with galactophoritis, but then postoperative pathological results showed there was mammarv duct ectasia complicated with galactophoritis in other galactophores. The symptoms vanished after a mammary duct endoscope-guided medicinal rinsing. Another 3 patients suffering from galactostasis were cured following 1~3 rinsings.
Purulent nipple discharge occurred in 6 cases, with a primary inverted nipple complicated with repeated abscess formation around the mammary areola. An incision and drainage operation was conducted on average once every 2 weeks or one per month, with a length of the case histories ranging from 6 to 24 months. The breasts were painful, and the patients even requested to have them removed. Examination of the abscess-effected quadrant was performed, and all results indicated an obstructive galactophoritis (OG). After mammary duct endoscope-guided rinsing 2 or 3 times, the patients healed well. They were advised to rectify the inverted nipples, and keep their nipples clean. No relapse occurred during the subsequent follow-up for 3 to 6 months.
In another 8 cases with yellow or colorless and transparent polyrrhea, one was confirmed as an intraductal papillomatosis by pathologic diagnosis, and all the other 7 were MDE and (or) galactophoritis. All patients healed following the mammary duct endoscope-guided rinsing for 1 to 3 times. After treatment in 2 of these patients complicated with a peri-areolar mass, the mass was significantly reduced or vanished (Fig.1).

A, Ultrasonic image before the treatment; the arrow refers to the subareolar effusions. A1,. The mass of intraluminal floccules obstructing a galactophore found by ductoscopy examination before treatment. B, Ultrasonic image one month after the ductoscopy-guided interventional therapy; the arrow means a significant minification of the focus with effusion. B1, After the ductoscopy-guided interventional therapy, the intraductal floccules were significantly decreased.
Discussion
Exclusive of systematic factors, refractory ND of non-lactating women usually indicates a structural lesion of the galactophore, in which some be a sign of an early intraductal tumor. ND can even be considered one of the primary symptoms of some breast cancers. Li et al.[4] found, following a retrospective investigation of 436 cases with nipple haemorrhage (NH) from 1978 to 1996, that there were 83 cases with Stage-T0 cancer, which were 19% of the total cases who received treatment for NH over the same period. These results suggest a need for high vigilance when ND occurs, especially with NH.
Xiao and Ya[5] reported on the studies by others using genetic analysis of mammary duct cells, that about 95% of breast cancers originate from these cells. Common precancerous breast cancer lesions occurring in oriental females are atypical ductal epithelial hyperplasia and duct papillomas. In China, breast cancers with an intraductal origin are the most common, usually with a single-duct origin and sole primary focus[6]. In our study, the proportion of intraductal space-occupying lesions (ISOLs) was significantly higher in those cases with BND compared to those with non-BND (*P < 0.025, **P < 0.001). A 3,000-case report by Xing et al.[7] suggested that there was a close correlation among yellow serosity, BND and IDP, and that the ISOL accounted for 90.2% of the BND cases. Therefore patients with a yellow and serous polyrrhea, and BND should receive maximal attention. Zhang et al.[8] analyzed the data from 354 cases with ND ductoscopy. They found that both benign and the malignant tumors have a definite proportion of polyrrhea of various compositions. Therefore they insist that all abnormal ND should be considered as an object of fiberoptic ductoscopy in women during their reproductive age or in a non-lactation period. Zhou et al.[9] proposed that BND has a potential of intraductal papillomatosis or breast cancer, and surgery is needed no matter the result of galactography or a ND smear. We found by examination of the mammary duct pores of patients with BND, that ISOL accounted for 81.8% of the BND cases, while the number of BND galactophores accounted for 75.0% of the total examined mammary duct pores. These results are similar to the reports in the literature, suggesting the necessity of ductoscopy. However, all of the BND patients do not need surgery. Xing et al.[10] suggested that there was a necessary internal association between galactostasis and the formation of ISOL. We should not neglect the treatment of the galactorrhea patients only because of their physiological condition, but should find the lesion and treat it in a timely manner after the ductoscopy. Examination of the galactostasis and yellow and serous polyrrhea cases have also been emphasized, with a necessary assessment of hypophysial functions before the examination. Except for systematic diseases, intraductal papillomatosis can also be found by fiberoptic ductoscopy.
It was reported that most of the ND patients displayed no ISOL, accounting for only 48% to 52%[11,12]. Ductoscopy may relieve 50% of the ND patients from a surgical procedure[7]. In our study, 37.9% of the total ND cases had ISOL. These comprised 13.9% of the examined galactophores. Ductoscopy provides information to develop a differential diagnosis of an intraductal lesion, to select a type of surgery and can permit a direct preoperative localization of the affected focus for patients whose tumor is un-palpable.
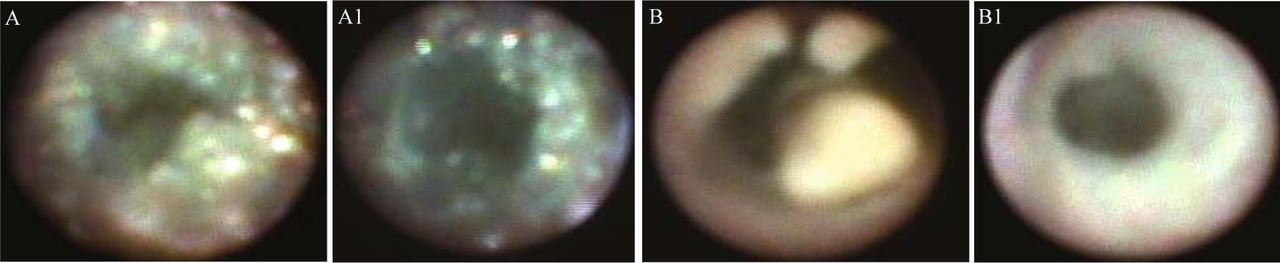
Of 2 patients in our group, one suffered from OG and the other from galactostasis. All results of the previous selective galactography before examination had suggested the possibility of BDP, so surgery preparation was needed. It was found via ductoscopy that there was extensive floccule and crystal-like stacking in one case, and a butyraceous accumulation in the other. ISOL was not seen in these 2 cases. After repeated washout of the diseased mammary ducts, reexamination showed that the intraductal floccules and crystal-like stacking significantly diminished, the cheese-like accumulation disappeared, and the polyrrhea ceased (Fig.2). Both patients were exempt from surgery.

A, OG before ductiscopy-guided treatment: a mass of floccules and crystal-like substance obstructed the galactophore in obstructive galactophoritis. A1, OG after one ductoscopy-guided treatment; the intraluminal floccules and crystal-like substance significantly diminished. B, Galactostasia: a mass of intraluminal butyraceous substance obstructing the galactophore. B1, Galactostasia: the intraluminal butyraceous substance disappeared, after only one ductoscopy-guided treatment.
In our study, iterventional ductoscopic rinsing was conducted in most of the patients suffering from galactostasis, galactophoritis, mammarv duct ectasia and repeated peri-areolar infection. After 1 to 3 medicinal rinsings, the ND abated and the mammary pain eased. Periareolar lumps disappeared in 2 cases. We believe that for the patients with bilateral and polyporous ND, an exclusion of the possibility of ND resulting from systemic or endocrine factors should be considered first. And then a ductoscopy ought to be conducted. It is best to examine the galactophores with ND respectively or by quadrants. Separate examination of a single ND galactopore is needed, in order to avoid missing a diagnosis. Fiberoptic ductoscopy has the merits of visualization and exact preoperative localization, eliminating unnecessary or excessive surgery, and lack of aversion to the technology. Most of the patients including those suffering from polyporous ND or mammary-duct disorders, especially the mammary duct patients with galactostasis, OG and MDE, achieved a thorough healing after the interventional ductoscopic medicinal rinsing.
- Received December 27, 2007.
- Accepted February 10, 2008.
- Copyright © 2008 by Tianjin Medical University Cancer Institute & Hospital and Springer
In this issue






{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.