

Abstract
OBJECTIVE To analyze the risk factors and influence of various treatments on the prognosis of non-Hodgkin’s lymphoma (NHL).
METHODS Clinical data of 92 patients with NHL from our hospital were retrospectively reviewed. Kaplan-Meier statistics were used to analyze the differences in survival times of the patients receiving various treatments. Cox regression model was employed for analyzing the prognostic factors.
RESULTS Among our patients, the 2 and 5-year disease-free survivals (DFS) were respectively 68% and 51%. The 5-year cancer-specific survival (CSS) was 55%. Mono-factorial analysis showed that the main independent prognostic factors included Ann Arbor Staging, B symptoms, lactate dehydrogenase (LDH), the international prognostic index (IPI) and age. Concerning the IPI, the 5-year CSS for the low-risk factors (0~1), lower-moderate risk (2), higher-moderate (3) and high-risk (4~5) were respectively 60%, 62%, 42% and 33%. Analysis of the prognoses, based on treatment of the patients with different stages, was as follows: the 5-year survival rates of the Stage-I and II patients, receiving surgery or chemotherapy alone, or a combined therapy, were respectively 19%, 72% and 68%, showing that the survival rates of the group with a combined therapy and the chemotherapy alone were superior to the group with surgery alone; the 5-year survival rates of the Stage-III and IV patients, receiving surgery or chemotherapy alone or a combined therapy, were respectively 50%, 35% and 60%, indicating that the survival rate of the group with a combined therapy was superior compared to the group with chemotherapy alone.
CONCLUSION Long-term survival of non-Hodgkin’ s lymphoma patients is closely related with multiple factors. Rational detection and assessment of the risk factors may prolong the living time of the patients. Different methods of treatment can influence the patient’s prognosis. Correct evaluation of the prognostic factors, and rational and effective therapy can prolong the patient’s survival.
keywords
Introduction
Non-Hodgkin lymphoma (NHL), which originates from the lymph tissue, is a malignant tumor that displays an extremely rapid infiltration and dissemination. Biological behavior and treatment methods vary greatly for the lymphomas of different types. Therefore assessment of the prognostic factors before treatment is crucial in working out and designing a reasonable and effective treatment plan. In this study, the influence of various risk factors on the prognosis and the significance of different treatment methods on the prognosis were investigated via a retrospective analysis and examination of NHL cases treated during the past years.
Material and Methods
General data
A total of 92 NHL cases from our hospital, during a period from January 1998 to December 2004, were collected, all of which were pathologically confirmed. Among all the patients, 59 were males and 33 females. Twenty-seven patients had an age of ≥ 60 years. General symptoms occurred in 56 patients (emaciation, night sweats, fever).
Clinical stages
Based on the Ann Arbor Staging, there were 14 cases with Stage-I NHL, 22 with Stage-II, 13 with Stage-III and 43 with Stage-IV. Upon admission, lymphatic infiltration was found in 64 of the total cases, and distant infiltration of one or more extra-lymphatic organs was found in 46 cases.
International prognosis index (IPI)
Scoring of the preliminary diagnosis was conducted based on 5 risk factors, i.e. the age (> 60 years), Ann Arbor Staging (Stage-I to IV), Performance Status Scoring (Ps ≥ 2), encroachment of multiple extra-lymphatic organs (> 1) and serum LDH level (≥ 500 IU/L). Each factor makes up one score, and grouping was carried out as follows: the low risk group (0~1 factor), lower-moderate risk group (2 factors), higher-moderate risk (3 factors) and high-risk group (4~5 factors).
Treatment
Twenty-one patients with extra-lymphatic lesions received simple surgery, and the other 25 patients with extra-lymphatic involvement received chemotherapy alone. The combined chemotherapy regimen usually included CHOP (CTX 650 mg/m2, i.v. drip infusion at d 1; ADM 30 mg/m2, drip infusion at d 1; VCR 1.4 mg/m2, drip infusion at d 1; and prednisone 60 mg/m2, oral administration during a period from d 1 to d 5), and CHOP plus Vpl6 treatment (i.e., the above regimen plus Vp60 mg/m2, with drip infusion in a period from d 1 to d 3). Forty-six patients without extra-lymphatic involvement received the combined therapeutic regimen, among which 5 also received a peripheral blood stem cell transplantation, following a complete remission as a result from the combined chemotherapy.
Statistical analysis
The overall survival time (OS) meant the period from the date of initial treatment to the date of death, final follow-up or deadline of observation. In our study, the observation deadline was August 10, 2005, and the main follow-up method was a follow-up visit by telephone. The Kaplan-Meier method was employed for calculating the survival rate, and Cox regression analysis was used to observe the effect of various clinical factors on the prognosis.
Results
Survival rate
There were 51 cases of death in our group that displayed 2 and 5-year overall survival rates of 52.6% and 23.7% respectively. For related survival rates associated with different prognostic factors, see Table 1. Mono-factorial analysis showed that the main prognostic factors of the NHL were the Ann Arbor Staging, B symptoms (fervescence, night sweat, emaciation), LDH, IPI and age. However, gender and extra-lymphatic involvement were not the important factors affecting prognosis, and there was no significant difference between the survival rates in relation with these factors.
Relationship between the 5 factors of 92 cases with NHL and the prognosis.
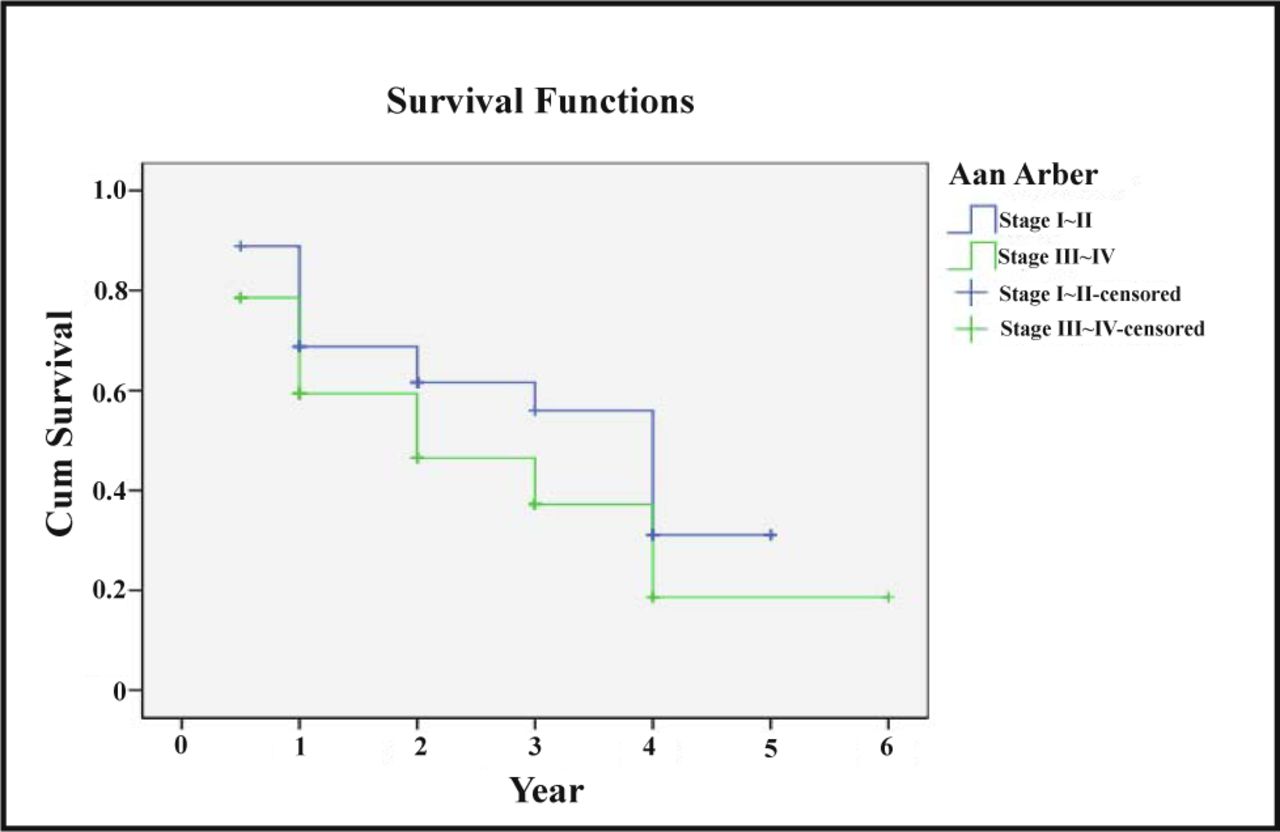
Staging and prognosis
Ann Arbor Staging was the key factor affecting the prognosis. The 2 and 5 year survival rates of Stage-I and II patients were respectively 59% and 28%, and those for the Stage-III and IV patients were respectively 46% and 13% (χ2 = 120.50, P < 0.05), see details in Fig.1.

Ann Arbor Staging and survival rate.
IPI and prognosis
Concerning the IPI, there were 30 cases with a risk of 0~1 score, 17 with a risk of 2, 20 with a risk of 3 and 25 with a risk of 4~5. The 2-year survival rates relating with these risks were respectively 62%, 60%, 51% and 36%, and the related 5-year survival rate were respectively 44%, 36%, 21% and 17%. There were very significant differences between the IPI and survival rates (χ2 = 27.12, P < 0.05). See details in Table 2 and Fig.2.
IPI and survival rate.
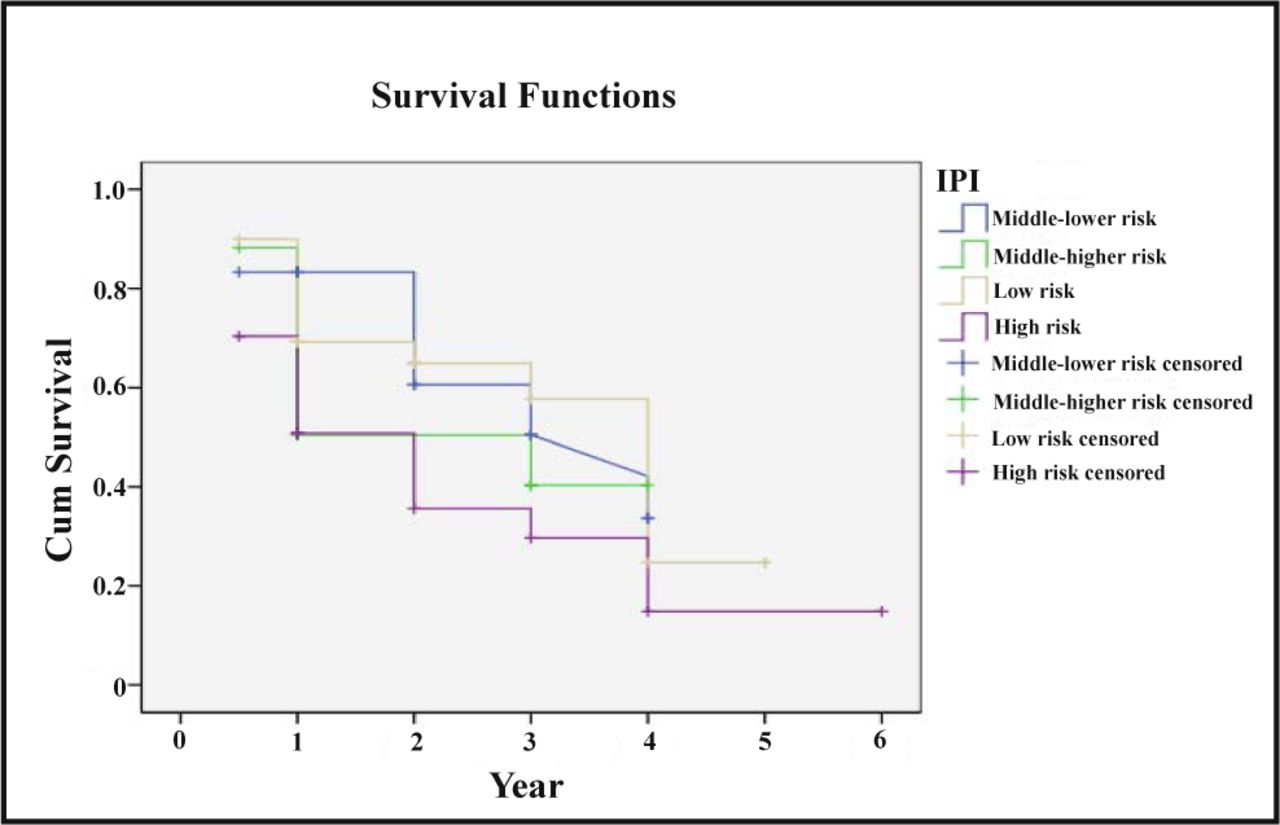
IPI and survival rate.
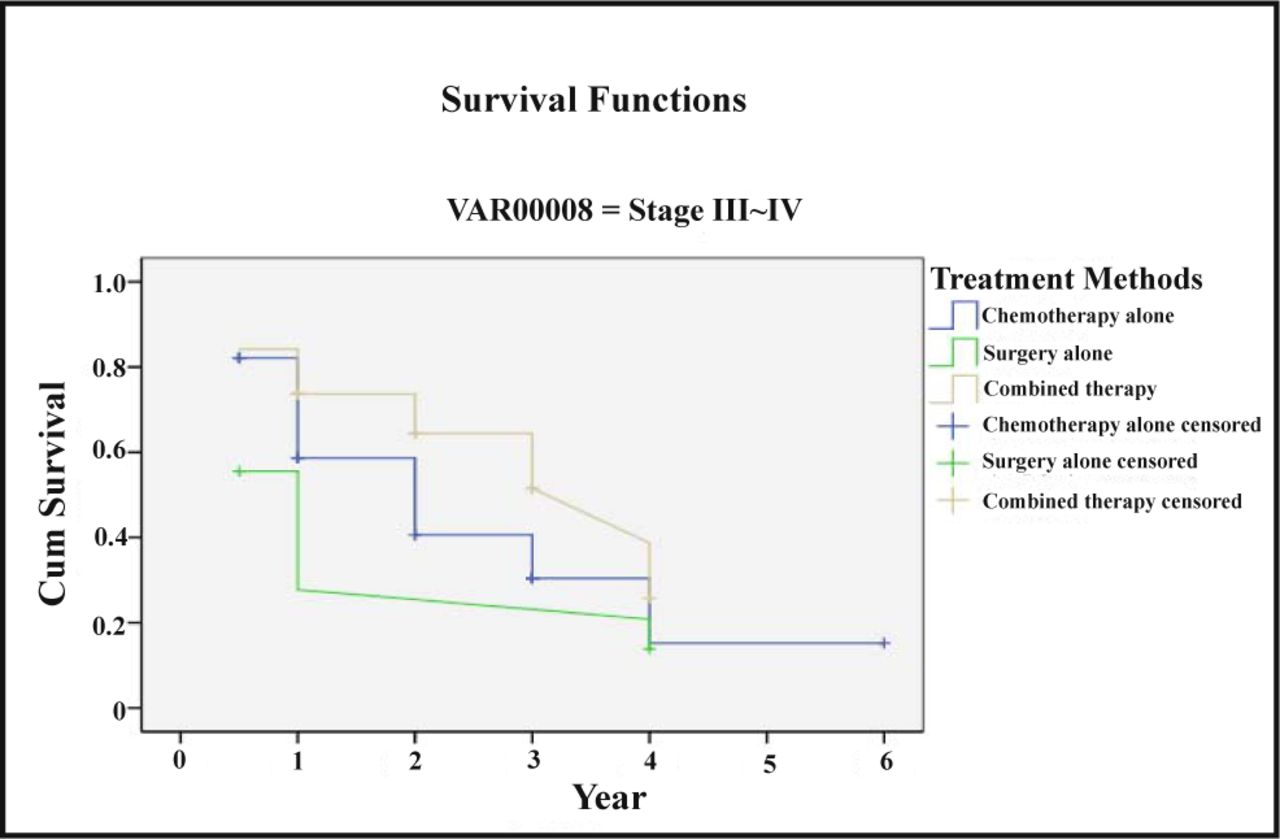
Treatment method and prognosis of patients with different tumor stages
The 5-year survival rates of all the Stage-I and II patients, receiving surgery alone, chemotherapy alone and combined chemotherapy, were respectively 0%, 58.3% and 42.9%. The 5-year survival rates of the Stage-III and IV patients receiving the same three treatments were 13.9%, 15.2% and 25.8% respectively. See Table 3 and 4, and Fig.3 and 4.
Treatment method and survival rate of Stage-I and II patients.
Treatment method and survival rate of Stage-III and IV patients.
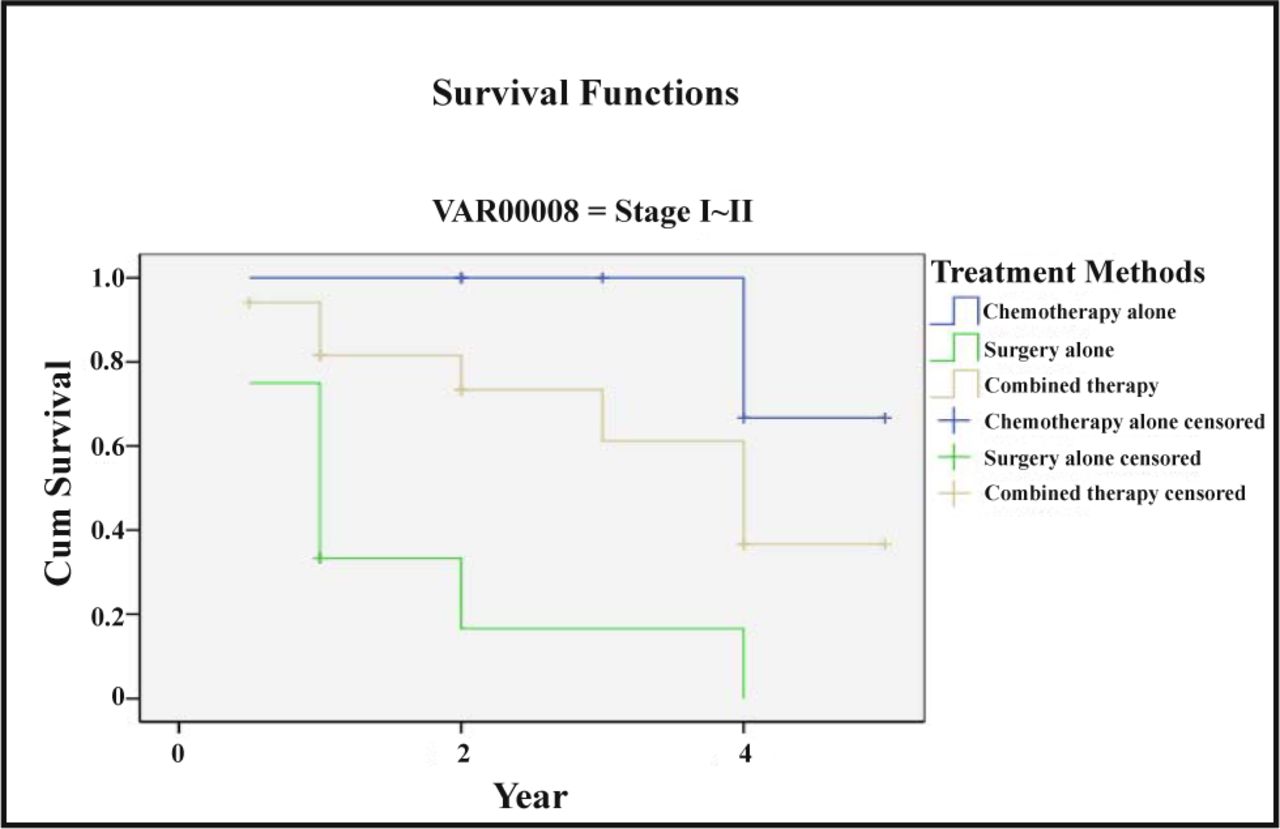
Treatment method and survival rate of Stage-I and II patients.

Treatment method and survival rate of Stage-III and IV patients.
Multi-factorial analysis
Cox regression analysis included sex, age, Ann Arbor Staging, extra-lymphatic involvement, general symptoms, LDH and IPI. Of the above mentioned factors, the Ann Arbor Staging, B symptoms, LDH, IPI and age were considered to be independent prognostic factors.
Discussion
NHLs are a group of heterogeneous malignant lymphomas. Their heterogenicity is mainly in relation to the pathological types, immunological phenotype and chromosomal caryotype. Our data show that prognosis of the NHL patients is closely correlated with multiple factors, which is in accordance with previous reports. Among so many factors, some are uncontrollable factors, such as gender, age and malignancy etc. Nevertheless some are controllable to a certain extent, such as early diagnosis and reasonable treatment etc.[1,2]
Relationship between prognosis of the NHL patients and IPI
It was thought, based on many past independent clinical studies[3], that a number of clinical factors would affect the prognosis of NHL, including age, the patient’ s physical activity, B symptoms, encroachment of multiple extra-lymphatic organs, invasion of bone marrow, Ann Arbor Staging, and the blood LDH level. From the data of our group, the Cox regression analysis indicated that the Ann Arbor Staging, B symptoms, LDH and age were independent prognostic factors. Gender and extralymphatic involvement had no relation with the prognosis. In the appraisement of NHL prognosis using IPI, the extra-lymphatic involvement of more than 1 score was one of the criteria. Although, based on our data, extralymphatic lesions had no relation with the prognosis, but it might relate to the lack of data and incomplete auxiliary examinations of some of the patients.
The NHL IPI group, after a multi-factorial analysis of 2000 plus cases who received adriamycin as the cardinal regimen, used the above mentioned factors to draw the conclusion that 5 factors, i.e. the age (of more than 60 years), Ann Arbor Staging (Stage-III and IV), performance status scoring (Ps ≥ 2), invasion of multiple extra-lymphatic organs (> 1) and serous LDH level (≥ 500 IU/L), were the major prognostic factors, and were called the NHL IPI. Based on the IPI, lymphoma cases were divided into low-risk, middle-lower risk, middle-higher risk and high-risk groups. The grouping played a definite role in prediction of the patient’s prognosis. Our findings showed that, based on the NHL IPI grouping, the 5-year survival rates of the low-risk, middle-lower risk, middle-higher risk and high-risk patients from the 92 NHL cases were respectively 44%, 36%, 32% and 17%. The survival rates gradually fell off, from the low-risk to high-risk groups, showing a statistically significant difference (P < 0.05). In the cases receiving the IPI investigations conducted by international NHL groups, the 5-year survival rate of the patients from the middle-lower risk group was 51%, and the 5-year survival rates of the patients from the middle-higher risk and high-risk groups were 43% and 26% respectively. The survival rates of the patients from the middle-higher risk and high-risk groups were especially low, which were similar to the findings of the IPI group. Therefore, the IPI appraisement of the first-visit patients is needed to as-certain the malignant degree, and to direct the choice of treatment plan, thus improving the therapeutic efficacy.
Relationship between prognosis of NHL patients and the treatment method
NHL is a common malignant tumor, with a year-by-year increase in the incidence rate over the past few years. Based on the pathological immune typing, most NHL cases are of the progressive type, such as the diffuse large-cell and the immunoblast types etc. A long-term remission may be attained in an approximately 30% or 40% of progressive-type NHL patients, who at present receive a conventional therapy (e.g. CHOP regimen). However, failure and relapse after the conventional therapy still occurred in about 60%~70% of the patients, and the effect of salvage treatment is poor. The key for improving the therapeutic efficacy is to identify high risk progressive-type NHL cases which have a poor curative effect with conventional therapy. This will enable application of a rational treatment with high intensity[3,4].
Concerning the treatment of NHL, it is now accepted that the COPP regimen or CHOP combined with interferon, can be used to treat patients with NHL of low potential malignancy, combined radio-chemotherapy for moderate Stage-I and II, and chemotherapy for the Stage III and IV NHL patients. The CHOP regimen remains as the treatment of choice for moderate NHL patients[5-7]. Our results indicated that the 5-year survival rates of the Stage-I and II NHL patients receiving chemotherapy alone, surgery alone, and combined therapy were respectively 58.3%, 0% and 42.9% (P < 0.05), and those with Stage-III and IV disease who received the three treatment methods were 15.2%, 13.9% and 25.8% (P < 0.05) respectively. The 5-year survival rate of the patients receiving combined therapy and chemotherapy was superior to that of the patients receiving surgery alone. The survival rate of the Stage-I and II patients receiving chemotherapy alone was superior to that of those patients receiving combined therapy. The main reason of this difference is that there were many advanced-stage cases in the combined-therapy group. The combined therapy included the regimen of surgery plus chemotherapy, chemotherapy plus radiotherapy, and transplantation. After complete remission by an induced chemotherapy, high-dose radio-chemotherapy combined with autogeneic or heterogeneic hemopoietic stem cell transplantation can markedly raise the long-term survival rate of the initially treated patients, who have unfavorable prognostic factors[8-10].
Based on our study, as soon as the final diagnosis is made, a strong and large-dose regimen of combined chemotherapy should be applied as early as possible for NHL patients who previously had a preliminary diagnosis. For the Stage-III and IV NHL patients, a chemotherapeutic regimen of 6 to 8 courses, or even more, should be conducted. Hemopoietic stem cell transplantation of Stage-III and IV patients is highly recommended, if the physical state of the patients permits. Early performance of high-dose chemo-radiotherapy, combined with hemopoietic stem cell transplantation, is necessary for the lymphoma patients of moderate and high potential malignancy, and refractoriness.
- Received December 10, 2007.
- Accepted March 27, 2008.
- Copyright © 2008 by Tianjin Medical University Cancer Institute & Hospital and Springer
In this issue






{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.