

Abstract
OBJECTIVE Traumatic neuromas are rare benign lesions occurring post-mastectomy, which are usually suspected as tumour recurrences before excision biopsy. We report six cases presenting with palpable nodules postmastectomy, to emphasize the differential diagnosis of traumatic neuroma from recurrent cancer.
METHODS Six cases were reviewed. The age of patients ranged from 33 to 61 years. Nodular masses were found close to the mastectomy scar during follow-up over a period of 2.8 to 8 years.
RESULTS In one patient three nodular masses were detected. Five patients had received chemotherapy, three of which had also received radiotherapy. Ultrasound examinations showed a well-circumscribed, homogeneous, hypo-echoic subcutaneous nodular lesion in four cases, and a poorly defined hypo-echoic nodule with good conduction in two cases. No obvious distant metastases had been identified. Each patient underwent surgical excisional biopsy. All of nodules had a diameter less than 1 cm. Histopathological examination showed proliferation of nerve fibre bundles, which were disordered, oriented and well circumscribed in fibro-adipose tissue.
CONCLUSION It was concluded that all of the lesions were traumatic neuromas, independent from the initial tumor. Traumatic neuromas occurring in mastectomy scars are difficult to distinguish from a tumor recurrence. Although radiological evaluation of the mass with ultrasound is of value, the diagnosis can only be confirmed following a histopathological evaluation.
keywords
INTRODUCTION
Most traumatic neuromas are the consequence of non-specific external injuries. Less commonly, traumatic neuromas have been described in scars after surgical procedures[1-3]. Traumatic neuromas are secondary to the disordered proliferation of nerves and connective tissue attempting to reinnervate the area after a total or partial sectioning of a nerve during an accidental or surgical trauma.. They are diagnosed some years after the trauma, usually by chance, as a small tumor near the scar that is tender to palpation or spontaneously painful[4].
We describe herein six cases of traumatic neuroma observed at the site of mastectomy scars. All these cases were chance findings during the follow-up of breast cancer patients with suspected tumour recurrences. Since traumatic neuromas are benign lesions, they must be distinguished in order to manage the patient’s treatment.
PATIENTS AND METHODS
Six patients, who were diagnosed with traumatic neuroma in our hospital after mastectomy, were reviewed. The diagnosis and treatment of the breast cancers were also studied. In the clinic, these patients, presenting with palpable nodules near a mastectomy scar, were suspected as having a recurrence. No obvious distant metastases had been identified. Surgical excisional biopsy was performed on each patient with histopathology confirming that these nodular masses were traumatic neuromas.
RESULTS
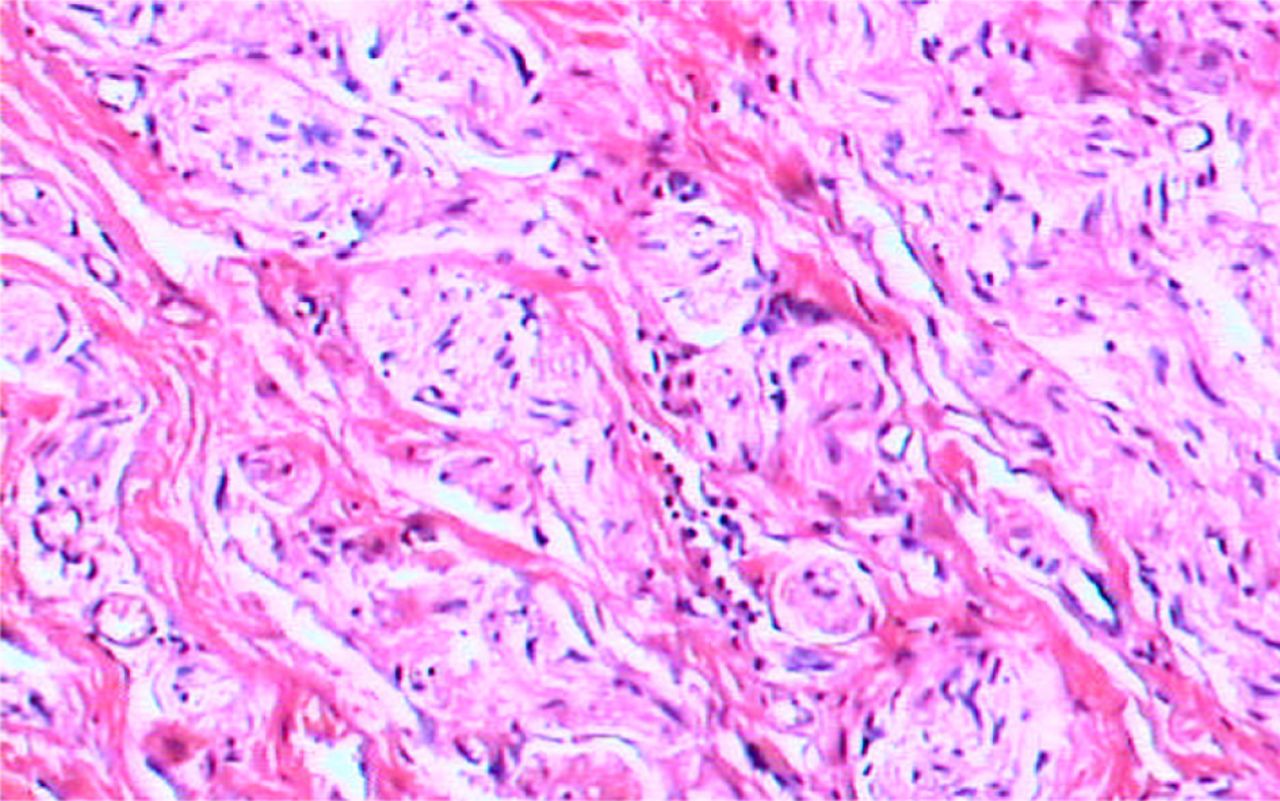
All six cases presented with palpable nodules near the mastectomy scar. The nodules were found either by a doctor or by themselves during follow-up of breast cancer surgery. The clinical features for each patient are shown in Table 1. The ages of the patients at the time of traumatic neuroma diagnosis (2.8 to 8 years after mastectomy) ranged from 41 to 68 years. Only one patient had three nodular masses near the mastectomy scar. The other five patients had only one nodule. Two masses were found close to the mastectomy scar, two were subclavicular and one was in the axilla. The masses were painless with diameters less than 1 cm in all cases. Ultrasound examinations showed a well-circumscribed, homogeneous, hypo-echoic subcutaneous nodular lesion in four cases and a poorly defined hypo-echoic nodule with good conduction in two cases. The patients were suspected as having a recurrent cancer. No obvious distant metastases were identified, so an excisional biopsy was performed on the presenting nodules. Histopathological examination showed proliferation of small nerve fibre bundles which disordered, oriented and well circumscribed in fibro-adipose tissue under the epidermis (Fig.1). It was concluded that they all were traumatic neuromas, independent from the initial tumor.
Clinical features for six cases of traumatic neuroma after mastectomy.
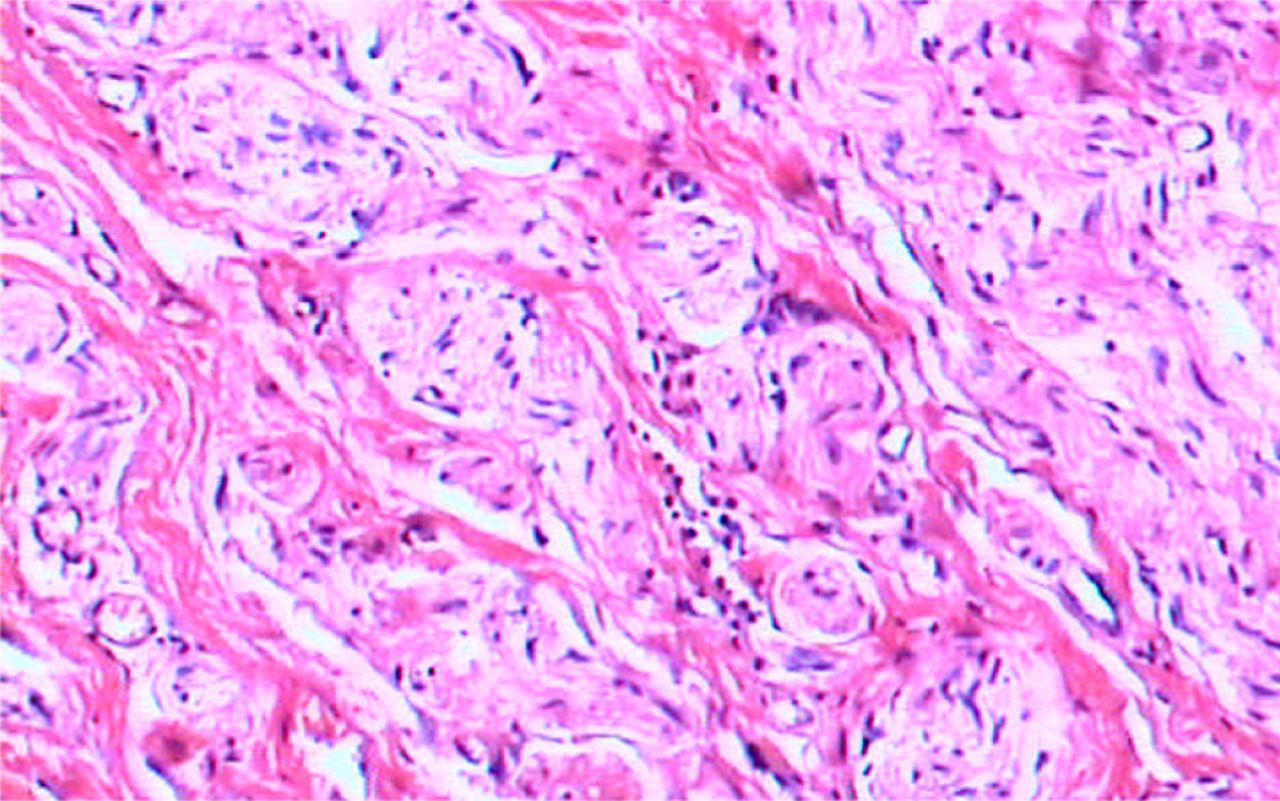
Small and medium size nerve fibre bundles, which were disordered, oriented and well circumscribed in fibro-adipose tissue (H & E stain, X100).
Table 2 shows the diagnosis and treatment for each patient. The ages of the patients at the time of diagnosis and mastectomy ranged from 33 to 61 years. Four patients had their tumor on the left side and two on the right side. There were two patients in each of following stages: T1N0M0, T2N0M0 and T2N1M0. All six patients were diagnosed by histopathology as invasive ductal carcinoma of the breast and all underwent either a radical or modified radical mastectomy. Five patients received chemotherapy three of which were treated with radiotherapy. Based on their ER and PR status, two patients were treated with tamoxifen for five years, and two patients are still being treated with tamoxifen.
The diagnosis and treatment of breast cancer for each patient.
DISCUSSION
An amputation or traumatic neuroma results from an attempt by an accidentally or surgically injured nerve to regenerate. When a nerve is transected, distal axons suffer Wallerian degeneration attributed to the inflammatory response, whereas the axons and Schwann cells of the proximal stump proliferate. Under normal conditions, the two segments eventually meet and the distal stump recovers innervation. However, if there is tissue between the stumps, e.g., scar tissue, or if the distal stump is lost, nerve proliferation continues from the proximal stump without finding its assembly point, producing a disorganized cell tangle composed of neural fibers and connective tissue that extends into the surrounding soft tissues until it forms an amputation neuroma[5].
Neuromas arising postoperatively following cancer surgery are not well established in the literature, unlike traumatic neuromas following excision for benign diseases such as a cholecystectomy[2, 3]. In an early study of neuromas occurring in cancer patients, 67 cancer patients presented with traumatic neuromas[6]. The most frequent site of a traumatic neuroma was at a radically dissected neck, followed by upper and lower extremities; only six patients with a radical mastectomy had traumatic neuromas. There were two published cases found of traumatic neuromas, which resembled granular cell tumors at mastectomy scars[7]. Additionally, a case report on traumatic neuromas occurring 2 years post-mastectomy showed that ultrasonographic examination and axial computed tomography imaging may help in a differential diagnosis from recurrence cancer[8]. Ultrasonography showed a well-circumscribed, homogeneous, hypoechoic subcutaneous nodular lesion[9]. Axial computed tomography images revealed a subcutaneous soft-tissue mass resembling a triangular form based on the pectoral muscle at the mastectomy scar region, showing a density similar to that of muscle attenuation. Several imaging techniques e.g. ultrasonographic, computed tomographic, and magnetic resonance imaging features have been used to differentiate traumatic neuroma from recurrent lymphadenopathy after neck dissection[10, 11].
Traumatic neuromas may cause pain, but many are asymptomatic; therefore, in a patient with pain at a site of amputation, other causes of the pain should be sought, e.g. infection or a tumor recurrence. The demonstration of a typical mass in the line of the transected nerve is diagnostic for traumatic neuroma. They usually do not exceed 2cm in diameter, are diagnosed between 1 and 10 years after surgery, and can be located in any organ. Although more frequent in peripheral sensory nerves, they can affect any motor or sensory nerve and even nerves of the autonomic nervous system[12]. In fact, the formation of amputation neuromas in sympathetic branches is not rare when the cystic duct is dissected during a cholecystectomy. Traumatic neuromas occurring in mastectomy scars are a distinct diagnostic problem that has been rarely reported in the literature. In our study we described six cases of traumatic neuromas after mastectomy, which are difficult to distinguish from a recurrent tumor. The excision of an amputation neuroma is justified when there is a suspicion of a recurrent tumor or a lymph node metastasis at this level, when it becomes painful, or when the patient requests it. Although radiological evaluation of the mass with ultrasound or computed tomography is of value, the diagnosis can only be confirmed with a histopathological evaluation.
ACKNOWLEDGEMENT
This work was supported by the Talented Professionals Scientific Research Fund of the Tianjin Medical University Cancer Institute and Hospital (6-28).
- Received December 12, 2006.
- Accepted May 3, 2007.
- Copyright © 2007 by Tianjin Medical University Cancer Institute & Hospital and Springer
In this issue






{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.