

Abstract
OBJECTIVE The present study was designed to evaluate the epidemiological and prognostic significance of proteinuria in patients with gastric cancer (GC).
METHODS We retrospectively reviewed the frequency of proteinuria in patients with GC and analyzed its relationship with the GC biological characteristics, treatment and survival.
RESULTS Proteinuria incidence in GC patients was 24.06%, which was significantly higher than that found in a control group (P<0.01 ); the frequency of proteinuria was significantly correlated with an advanced disease stage (P<0.01). We also found that the post-treatment mean value of proteinuria was remarkably lower than the pre-treatment value (P<0.001). Kaplan-Meier analysis revealed a significant correlation between proteinuria and survival of GC patients (P<0.05). Multivariate analysis demonstrated that the TNM stage, lymph node status and proteinuria may serve as independent prognostic markers in patients with GC (P <0.01 ).
CONCLUSION A high prevalence of increased urinary protein excretion was observed in GC patients complicated with nephritis. Proteinuria may be used as one of the prognostic markers for patients with GC.
keywords
The presence of proteinuria in cancer patients was first noted by Lee et al.[1] Since that time, other investigators have confirmed this relationship and also reported that a minimal increased urinary albumin excretion rate was frequently observed in patients with different malignant diseases. According to Keur, the incidence of a glomerulopathy in cancer patients varies between 3 and 13% with a mean of 7%.[2] The most common malignancies are located in the blood, lung, gastrointestinal tract, prostate, breast and ovary, etc. Proteinuria can be used as an important prognostic marker to evaluate survival in patients with malignancies. Pederson indicated that patients with microalbuminuria have a significantly lower survival rate compared to a group of patients with normalalbuminuria.[3] The prevalence and prognostic significance of the nephritic syndrome, however, have never been described previously in gastric cancer (GC) patients. In the present study, we retrospectively collected 320 GC cases admitted to our hospital from 1995 to 1998 to investigate the association between proteinuria and prognosis in GC patients.
Materials and Methods
Clinical data
The study population consisted of 320 patients (male: 197; female: 123) who were diagnosed with GC in our hospital between 1995 and 1998. The mean age of the patients was 51.3 years (range: 35~63 years). Histological examination indicated that of the 320 cases, 256 belonged to a differentiated type and 64 to an undifferentiated type; there were 59 cases with and 261 without lymph node metastasis. All the patients underwent surgery and were followed-up for more than 5 years. The study also constituted of a control group of 123 patients (male: 74, female: 49) with benign gastric disease diagnosed over the same time period. Mean age of these patients was 55.1 years (range: 32~66 years). The pathology of the 123 cases included 38 benign ulcer, 27 chronic superficial gastritis, 49 chronic atrophic gastritis and 9 benign tumors. Patients with primary and other secondary diseases that could result in proteinuria, such as diabetes mellitus, hypertension, cardiac asthma, immune system disease and urinary tract infection, were all excluded from the study.
Criteria and methods
The GC pathological type was confirmed by pathological examination for the specimen obtained from biopsy and operation. The classification was conducted according to the WHO gastric cancer international staging system, and the TNM stage according to UICC (1987). Benign foci were confirmed by gastroscopic or pathological examination of the specimen. Proteinuria concentration was measured by a revised biuret method, with the value described as x ± s. A proteinuria of > 150 mg/24hr was defined as positive, <150 mg/24hr as negative. Proteinuria was determined for the 320 GC patients and 123 controls at the time of primary diagnosis. Seventy-seven GC patients with positive proteinuria at the time of diagnosis were also tested after 2 months of treatment. Analysis for 1~5 year survival rates for the GC patients was performed.
Statistical methods
Comparison of proteinuria between patients with GC and those with benign gastric disease, as well as with different TNM stages were analyzed with the x2 test. For the GC patients with positive proteinuria at the time of diagnosis, a paired t-test was used to compare the pre-treatment and post-treatment proteinuria. Survival curves were calculated according to the Kaplan-Meier method and compared using the log-rank test and COX multivariate analysis.
Results
Comparison of proteinuria between GC patients and the controls
As shown in Table 1, the positive rate of proteinuria in GC patients was significantly higher than that in the controls (P<0.01).
Incidence of proteinuria in GC patients with different TNM stages
As shown in Table 2, the total positive rate of proteinuria was 13.08% for patients in stages I plus Hand 29.58% for patients in stages III plus IV. Patients with advanced disease (III and IV) had a significantly higher positive proteinuria rate than patients with localized disease ( I and II, P<0.01).
Comparison of proteinuria between pre-treatment and post-treatment
For the 77 cases with positive proteinuria at the time of diagnosis, the post-treatment mean value of proteinuria was significantly lower than the pre-treatment mean value 1467 ± 78 tng/24 h vs 865 ± 46 mg/24 h ( P < 0.001).
Comparison of the 1~5 year survival rates between 77 GC patients with proteinuria and 243 without proteinuria
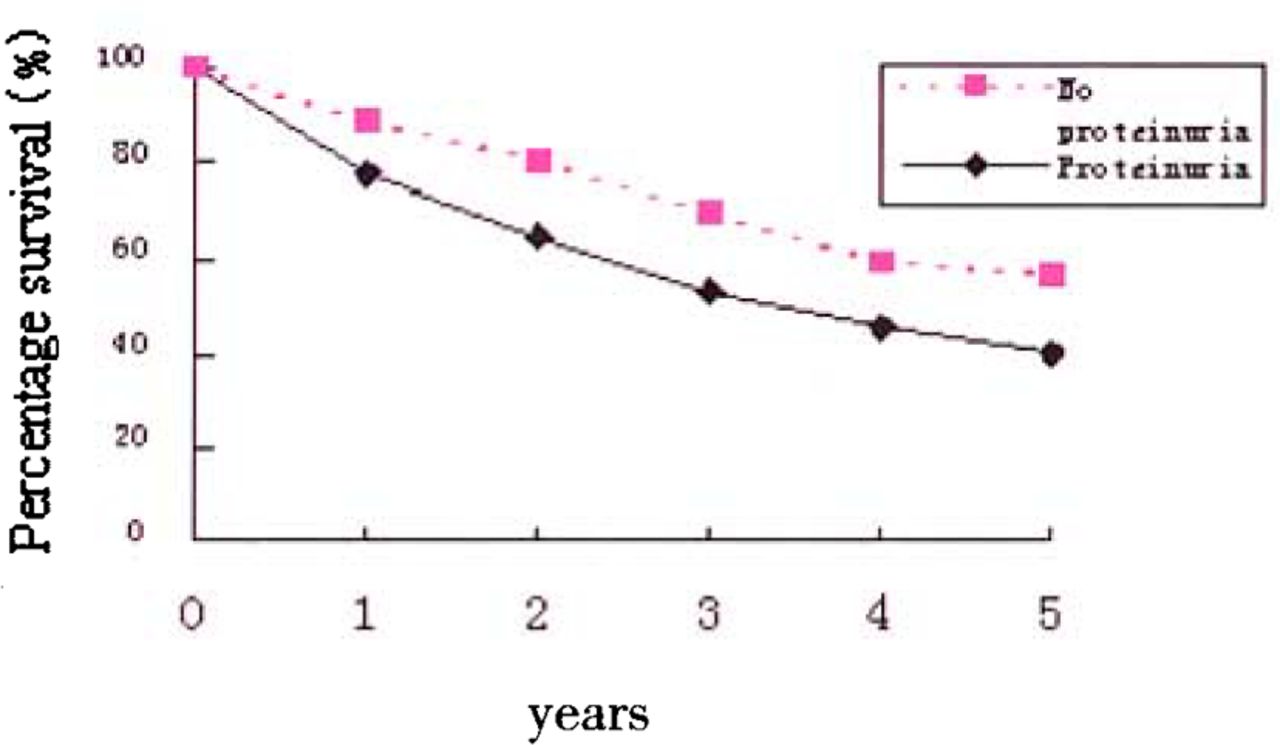
Survival curves according to the proteinuria level described by the Kaplan-Meier method are shown in Fig.l. The log-rank test indicated that the 1~5 year survival rates for GC patients with proteinuria were 77.92%, 64.94%, 53.25%, 45.45%, 40.26%, respectively, and for patients without proteinuria at the first diagnosis, the values were 88.48%, 80.25%, 69.55%, 59.26% and 56.38%. The difference between the two groups was significant (P<0.05).
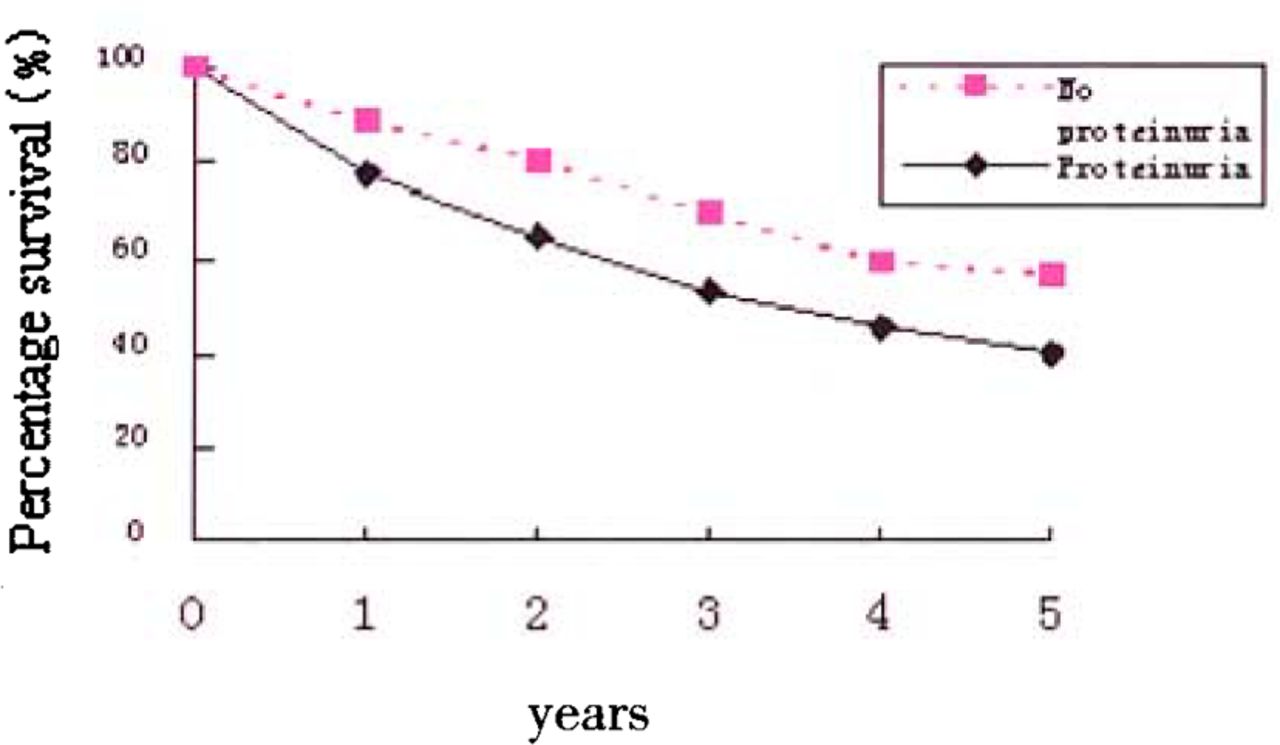
Comparison of survival rate between GC patients with and without proteinuria.
Analysis for prognostic factors
The log-rank test demonstrated that survival of GC patients was influenced by the age, proteinuria, TNM stage, histological type and lymph node status etc. As indicated in Table 3, COX multivariate analysis further showed that TNM, lymph node metastasis and proteinuria were significantly correlated with GC patient survival (P <0.01) These associations can be regarded as independent prognostic indicators, while no relationship of prognosis with gender, age or histological type was found.
Discussion
Renal damage resulting from malignancies had been recognized as early as the 19 century. With an increase in the population of elderly people and environmental pollution becoming more serious, the incidence of cancer has risen, resulting in more attention to tumor-associated kidney damage. Since malignancy-associated nephritis was first noted by Lee et al. in 1966, [1] many investigators have studied nephritis associated with hematogenous tumors, lung cancer and gastrointestinal cancer. Recently, there have been several reports on nephritis resulting from metastatic prostate cancer and transitional cell carcinoma of the urinary bladder, [4,5] IgA nephropathy from esophageal basaloid squamous carcinoma,[6] pulmonary and renal amyloidosis associated with cutaneous squamous cell carcinoma, [7] rapidly progressing glomerulonephritis with carcinoma of the hypopharynx[8] and membranous nephropathy with pleural mesothelioma,™ etc. Among all the malignant tumors, epithelium-originated carcinoma holds the most significant correlation with nephritis. The present study demonstrated that the incidence of GC associated with proteinuria was 24.6%, higher than the mean value reported by Keurl et al., [2] which may be related to the biological characteristics of GC and case selection. The possible mechanisms of renal injury associated with malignant tumors include the following aspects: (1) direct invasion; (2) tumor-associated abnormal metabolism, such as hypercalcemia, hyperlithuria and hypokalemia; (3) damage due to treatment, such as radiation nephritis; (4) immune response-induced glomerulonephritis, namely tumor-associated nephritis; (5) other factors. In our study we have emphasized tumor-associated nephritis, which was extensively accepted as inflammation damage induced by immune complexs. The possible antigens include (1) tumor-associated antigens; (2) reappearing oncofetal antigens; (3) viral antigens; and (4) nontumorigenic autologous antigens. The pathological type of tumor-associated nephritis depends on the original tumor. The most common nephritis is membranous nephropathy, with a proportion of 60~70%. The other types involve focal segmental glomerulosclerosis, membranoproliferative glomeru-lonephritis, minimal change, glomerulonephritis and crescentic glomerulonephritis.[10]
The main manifestations of tumor-induced kidney injury are glomerular proteinuria and even developing into the nephritic syndrome (NS). Besides, hematuria and hypertension, acute or chronic renal failure can also occur in cancer patients. It was reported that the NS manifested itself one year prior to or concomitantly with the diagnosis of the neoplasm in approximately 80% of the cases. So NS patients over 40 years of age should be regarded as possibile cancer pateints. About 10% of NS patients over 40 developed carcinoma rapidly or in 14 months after they were diagnosed with the NS. In patients over 60 years of age, the incidence was as high as 22%.[2,11]
Our results indicated that the total proteinuria incidence in patients staged as I and II was significantly higher than that in patients staged as III and IV. Patients with advanced disease had a higher proteinuria incident rate, suggesting different renal damage in different cancer stages. Thus, patients with metastatic or advanced carcinoma should be treated with an awareness of possible renal damage initiation.
In accord with our current study, Pederson and Sorenson showed that median urinary albumin excretion was significantly higher in patients with metastatic breast cancer compared with the early breast cancer group. [3] These results may be related to intensified damage of the glomerular filtration membrane, resulting from tumor cell metabolite overexpression, immune monitoring deficiency and/a immune system injury, etc.
Effective treatment may reduce proteinuria excretion in cancer patients. According to Ashman et al, a bronchial carcinoid patient was successfully treated with combined chemotherapy and radiotherapy, and over the period his NS resolved.[12] Reshi et al. reported that proteinuria in a transitional bladder carcinoma patient associated with NS disappeared 4 weeks after the removal of the tumor.[5] Hematogenous proteinuria is more sensitive to chemotherapy and radiotherapy.[13]We found that the post-treatment mean value of proteinuria was significantly lower than the pre-treatment mean value. Since chemotherapy and radiotherapy alone can lead to renal damage, proteinuria and renal function should be periodicly assessed during clinical treatment.
The presence of proteinuria in patients with a malignant tumor with associated nephritis has important epidemiological and clinical significance, which was reaffirmed by the present study. Due to a significantly lower survival rate of GC patients with proteinuria compared to non-proteinuria GC patients, proteinuria can be used as an independent indicator to estimate GC patient survival. The possible explainations of the relation to survival consist of immune fonction disorders, malnutrition, endocrine malfunctioning, etc. More research, however, is warranted to elucidate other possible mechanisms.
For GC patients associated with NS, it is necessary to perform combined treatment for cancer and renal damage to avoid metabolic disorders, such as hypercalcemia with complicated hypokalemia. Effective infection control, improvement of hypovolemia and shock, proper chemotherapy and radiotherapy, avoiding renal-toxic drugs, elimination of factors that can intensify renal injury, such as hypertension, hyperperfusion and hyperfiltration and reduction of proteinuria excretion are all important for the cancer patients associated with NS.
Based on the present study and other reports, we reaffirm that there is a high proteinuria incidence in GC patients, and that there is a close relationship between proteinuria and GC biological characteristics. Patients with cryptogenic proteinuria, especially elderly people, should be examined to ascertain whether there is a tumor present. Reasonable anti-tumor therapy decreases proteinuria excretion. Therefore by attaching importance to the proteinuria incidence and by using proper supplementary therapy will add to the survival and quality of life the patients with GC. Proteinuria can be regarded as an independent risk factor in evaluating potential survival of GC patients. Association between other malignancies and prognosis needs further investigation.
- Received October 8, 2004.
- Accepted January 27, 2005.
- Copyright © 2005 by Tianjin Medical University Cancer Institute & Hospital and Springer
In this issue






{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.