

Abstract
Lymphoma rarely occurs during pregnancy, making this condition difficult to define. Lymphomas that occur in reproductive organs during pregnancy exhibit unique clinical characteristics. Among the limited cases, non-Hodgkin's lymphoma (NHL) shows a considerably higher incidence rate than Hodgkin's lymphoma (HL); NHL also displays clinical characteristics, such as high aggressiveness, advanced stage, and poor outcome. This study reports on four cases of lymphomas in non-gonadal organs (HL, n=2; NHL, n=2) during pregnancy. The tumors rapidly progressed in all patients during pregnancy but remitted at the end of pregnancy and/or therapy. The two HL cases were nodular sclerosis classical HL and treated with chemotherapy after terminating the pregnancy. One of the NHL cases was primary cutaneous follicular center lymphoma, a B cell-derived indolent lymphoma. The patient was followed up without any therapy after terminating her pregnancy. The other case was a follicular lymphoma grade 3B, which was treated with chemotherapy after delivery. We also conducted a literature review of 165 lymphoma cases occurring during pregnancy reported from 1976 to 2013 to reveal the correlation between pregnancy and lymphoma progression. Immunohistochemistry studies were performed to determine the expression of estrogen/progesterone receptors (ER/PR), and ER was weakly positive and sporadic. We concluded that lymphomas occurring during pregnancy should be managed with a prompt and reasonable treatment. High estrogen level in maternal body may affect lymphoma progression.
keywords
Introduction
The occurrence of malignant tumors during pregnancy gradually increases in women at reproductive age, and lymphoma ranks the fourth among the gestational tumors1. Lymphoma rarely occurs during pregnancy, with an incidence rate in 1 of 6,000 deliveries or fewer2–4. Lymphoma during pregnancy is easily neglected or misdiagnosed, and this tumor often grows and deteriorates rapidly, and even directly threatens the patients’ lives. The present report describes four cases of lymphomas in non-gonadal organs during pregnancy and provides a systematic review of the available literature.
Case reports
Case 1
Case 1 involves a 30-year-old patient showing a right-side supraclavicular mass at the fifth week of gestation. Ultrasound showed enlarged multiple lymph nodes. The patient decided to continue her pregnancy and was closely observed. During the 4 months of pregnancy, the mass increased progressively with time and the patient suffered from pruritus all over her body, low-grade fever, night sweating, and weight loss. Radiologic imaging revealed multiple enlarged lymph nodes below and above the bilateral clavicle and in the bilateral axillary and mediastinum. The largest lymph node in the left axillary measured 2.4 cm × 1.4 cm. The right-side supraclavicular lesion was resected immediately. Pathological examination showed effaced lymph node architecture, and lymphoid tissues displayed grown nodules wrapped with collagen. The background cells were mainly small lymphocytes and eosinophils, and large neoplastic cells were atypical Hodgkin and Reed-Sternberg (HRS) cells, which showed large prominent nucleoli and abundant cytoplasm ( Figure 1A and B). Immunostaining results indicated that these cells were positive for the cluster of differentiation 30 (CD30), weakly positive for PAX-5 (Figure 1C and D), and negative for CD20, CD15, LCA, CD3, and EBV-encoded RNAs in situ hybridization (EBER). The patient was finally diagnosed with nodular sclerosis classical Hodgkin's lymphoma (NSCHL). After discussion with the patient, her pregnancy was terminated and a standard chemotherapy (adriamycin, bleomycin, vinblastine, and dacarbazine, ABVD) was administrated. The patient survived and displayed complete remission (CR).
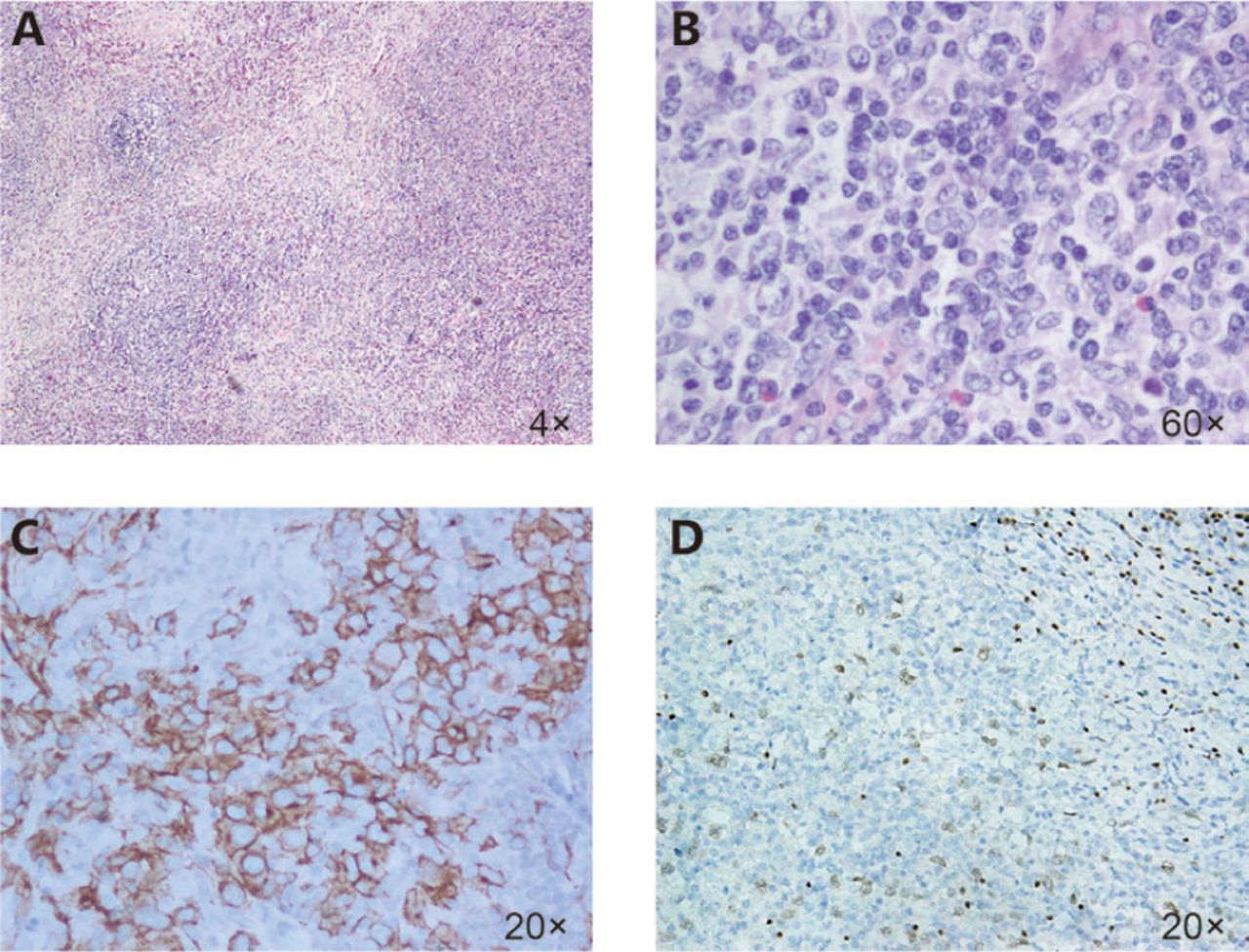
Hematoxylin and eosin (A, B) staining of the lesion and representative immunostaining images (C, D). Lymph node architecture was effaced and lymphoid tissues showed collagen-wrapped nodules. Neoplastic cells were atypical HRS cells showing small lobes, few prominent nucleoli, and dominant cytoplasm. Predominant small lymphocytes and eosinophils were observed. Typical immunostaining of CD30 (C) and PAX-5 (D) is shown.
Case 2
Case 2 involves a 25-year-old patient showing a right-side supraclavicular mass with 3.0 cm diameter at the fifth week of gestation; the tumor grew progressively within the past 15 days. Imaging examination showed enlargement of the anterior mediastinum and right supraclavicular lymph nodes. Core biopsy analysis of the enlarged lymph nodes revealed a small amount of abnormal cells dispersed in the inflammatory background. The right-side supraclavicular mass (5 cm × 4 cm × 3 cm) was removed surgically. Pathological examination revealed the morphology of collagen-wrapped nodules. A large number of classical Reed-Sternberg (RS) and RS-like cells displayed typical appearance on the background of eosinophils, abscess, and necrosis (Figure 2A and B). Neoplastic cells were apparently CD30+ and PAX-5+ (Figure 2C and D), but CD15-, CD20-, CD3-, LCA- and EBER-. The patient was diagnosed with NSCHL, and her pregnancy was interrupted. The patient then underwent chemotherapy cycles using the ABVD protocol. She displayed CR for 1 year after completion of the treatment.

Morphological features of the lesion. Lymph nodes contain collagen-wrapped nodules. A large number of classical RS and RS-like cells were observed at the center of the nodules, surrounded by eosinophils, and abscess formation and necrosis are occasionally spotted (A, B). Immunohistochemistry showed that the neoplastic cells were positive for CD30 (C) and PAX-5 (D).
Case 3
Case 3 involves a 36-year-old patient, who had a very small stable mass in the left inguinal region in November 2010. The mass was mistaken as an inflammatory hyperplasia nodule and was not given further attention. After 1 year when she became pregnant through artificial insemination, the small mass started to grow. The mass increased progressively from 2.5 cm to 9.0 cm in diameter from February to April in 2012; as such, spontaneous abortion occurred. Computed tomography (CT) analysis revealed a superficial tumor of the skin layer, which was removed surgically. Histological investigation showed a diffuse lesion in the subcutaneous lymphoid tissue, with nodules surrounded by fibroblasts and collagens. The neoplastic cells grew along the surrounding cutaneous appendage. Although most of the cells were small and medium in size, large cells were also observed (Figure 3A and B). Immunohistochemistry indicated that the neoplastic cells were positive for CD20 and Mum-1 but negative for CD10, BCL6, BCL2, CD3, CD5, and CyclinD1. Ki-67-positive cells were fewer than 5%, indicating a low proliferative rate of the tumor cells (Figure 3C and D). The patient was diagnosed with primary cutaneous follicular center lymphoma (PCFCL). No indications for chemotherapy were observed after considering the indolent course of the disease and comprehensive assessment of the patient. After 2 years of follow-up, the patient showed CR and had no systemic recurrence.

Diagnostic pathology and biopsy demonstrate a diffuse region with nodules surrounded by fibroblasts and collagens. The neoplastic cells grew along the surrounding cutaneous appendage. The cells were mostly small and medium in size, and the large cells were sporadic (A, B). Immunohistochemistry showed that most of the cells were strongly positive for CD20 (C), whereas cells fewer than 5% were Ki67-positive (D).
Case 4
Case 4 involves a 20-year-old patient, who presented with an enlarged mass of approximately 1.0 cm in diameter in the right side of her tonsil after 28 weeks of gestation. The mass was initially mistaken as tonsillitis but enlarged obviously with time. The patient decided to continue her pregnancy and refused any diagnostic procedure and treatment to protect the fetus in its advanced development. The patient finally delivered a healthy baby through cesarean section. One month after delivery, the patient went to see a doctor because of difficulty in breathing, weakness, and weight loss. The enlarged mass (approximately 3.5 cm in diameter) in the right-side tonsil was surgically removed. Pathological examination indicated that the remnant of normal tonsil tissues still exists. However, the lymphoid tissues contain irregular nodules and follicles, which predominantly comprised B-cell centroblasts. The neoplastic cells grew in patches, showing conspicuous and mitotic nucleoli (Figure 4A and B). Immunohistochemically, the tumor cells were B-cell associated antigens and positive for CD20, CD79a, BCL2, BCL6, and CD10 positive; the residual cells were identified as CD21+ follicular dendritic cells. Ki67 was expressed in more than 80% of the cells (Figure 4C-I). The cells were negative for CD3, CD5, CD38, CyclinD1, CD30, ALK, and EBER. The patient was diagnosed with follicular lymphoma grade 3B (FL3B). PET/CT scan indicated the implication in her neck, nasopharynx, and multiple lymph nodes. The patient is currently in CR after treatment with standard chemotherapy of rituximab and cytoxan, hydroxyrubicin, oncovin, and prednisone, with radiotherapy protocol on cycle regimen, followed by immunotherapy for supportive therapy.

Histopathological and immunohistochemical features of the tonsil. Lymphoid tissues showed irregular nodules and follicles, which composed predominantly of centroblasts. The neoplastic cells grew in patches showing conspicuous and mitotic nucleoli (A, B). Immunohistochemically, the tumor cells were positively stained for CD20 (C), CD21 (I), BCL2 (D, E), and BCL6 (G, H), whereas the staining of Ki-67 revealed a high proliferative rate of higher than 80% (F).
Discussion
The ages of patients at the onset of lymphoma are widely distributed and include the reproductive ages. Lymphoma during pregnancy is defined as a tumor occurring or discovered during gestational period. The lymphomas in all cases reported in this work were discovered and diagnosed during gestation. The occurrence of lymphomas and pregnancy is more likely a coincidence.
Lymphomas rarely occur in pregnant women, and only approximately 165 cases were reported from 1976 to 2013 as revealed by our systematic literature search. Among them, 110 cases were NHL and 50 cases were HL; no histological information was available in 5 cases. Only 24 cases were reported in China (NHL, 21; HL, 1; unclassified cases, 2), and diffuse large B-cell lymphoma is the most common subtype. Thus, the pathological types of lymphomas during pregnancy are not different from those found in non-pregnant women. A recent study has reported the occurrence of NHL in 121 patients during pregnancy from 1967 to 2012; 95% of them showed aggressive lymphomas and only 5% showed indolent lymphomas5. This paper reports on four cases of lymphomas occurring during pregnancy, two of which were NSCHL and the other two cases were B-NHL (PCFCL and FL3B). Horowitz et al.5 have found that NHL during pregnancy exhibits a unique clinical feature and involves reproductive organs, such as breast, ovary, and cervix uteri. Lymphomas in these four cases occurred in non-gonadal organs. Lymphoma during pregnancy generally can attack any organ; possibly, gonadal organs are usually involved.
Among the four cases, only one patient was diagnosed with aggressive lymphoma (FL3B), and the patient achieved CR under standard treatment. By contrast, the tumors in the three other patients progressed rapidly during pregnancy, even in the B cells-derived indolent lymphoma; this characteristic was a significant feature of these cases. The third case did not receive any treatment but achieved CR after terminating her pregnancy.
Developing a prompt and reasonable chemotherapy based on clinical stage, histological type, duration of pregnancy, and the risk of lymphoma is necessary to treat lymphoma during pregnancy. Some patients had delivered healthy babies despite receiving prenatal chemotherapy. Choosing the best time for chemotherapy is certainly important. Studies have suggested that standard chemotherapy regimens for lymphoma (without anti-metabolic drugs) should be administered during the second and third trimesters6,7. Among the four cases, one patient received tumor resection and was diagnosed with FL3B (an aggressive lymphoma) after delivery; the chemotherapy was thus deferred postpartum. Additionally, the PCFCL patient continued her pregnancy without any treatment, and her tumor grew rapidly, and spontaneous abortion occurred at the 6th month of gestation. The treatment for lymphomas within the first 12 weeks of gestation remains controversial. Some studies have suggested that early pregnancy should be terminated. A therapeutic abortion is the best conservative treatment because implementation of radiotherapy and chemotherapy during this period may cause unpredictable long-term effects on the fetus and/or may increase the risk of bleeding2,8. In the second case, pregnancy of the patient with NSCHL, which was discovered during the first trimester, was interrupted. By contrast, the diagnosis and treatment of the other NSCHL case were both deferred to the second trimester. The treatment strategy of ending the pregnancy, which was the choice of the patient, was insufficient. Interrupting the pregnancy of lymphoma patients in the metaphase and terminal gestational periods is generally unnecessary. Therefore, pregnant patients with high risk of clinical scenarios (aggressive lymphomas or progressive indolent lymphomas) should be managed concurrently with maternal-fetal medical consultation and must receive chemotherapy as soon as possible to protect maternal health and reduce harm to the fetus.
The clinical characteristics of lymphoma during pregnancy are apparently different from those of lymphoma found in non-pregnant women, which raises the question on whether a potential link exists between pregnancy and lymphoma. Some literature has indicated that the course of lymphoma is apparently affected by the changes in hormone levels during pregnancy9,10. A high level of sex hormone can stimulate reproductive organs during pregnancy. Additionally, sex hormone, especially estrogen, obviously influences some tumors in the reproductive system, such as breast cancer, endometrial carcinoma, and ovarian cancer. Estrogen and progesterone may also play an important role in the genesis and development of gonadal organ lymphomas. Most of the effects of estrogen/progesterone are mediated by their receptors: estrogen receptor α/β (ERα/ERβ) and progesterone receptor (PR). Therefore, immunostaining of ER/PR was performed in the four cases. ER expression is sporadic and weakly positive (Figure 5A and B) in case 2, whereas few cells expressed ER in the other three cases. PR is hardly positive (Figure 5C). Data showed that ERα and ERβ were identified in human normal lymphocytes and lymphoid malignancies, such as acute lymphoblastic and myeloma cell lines, chronic lymphocytic leukemia (CCL), HL, and NHL11,12. ERβ is the predominant type of ER in mature lymphocytes13. Yakimchuk et al.14 have demonstrated that ERβ is found in B-lymphocytes, and ERβ expression is upregulated in CLL. Our study found that immunostaining for ER in the cases was basically consistent with those reported. Cookman et al.15 have suggested that BCL2 expression in lymphocytes is functionally upregulated by estrogen. BCL2 is an important organelle-associated anti-apoptotic gene product, which inhibits apoptosis by blocking certain signaling transduction pathways. BCL2-positive tumor cells were observed (Figure 5D) in the two NSCHL cases. ERβ may upregulate some factors to actively inhibit apoptosis and increase growth15.
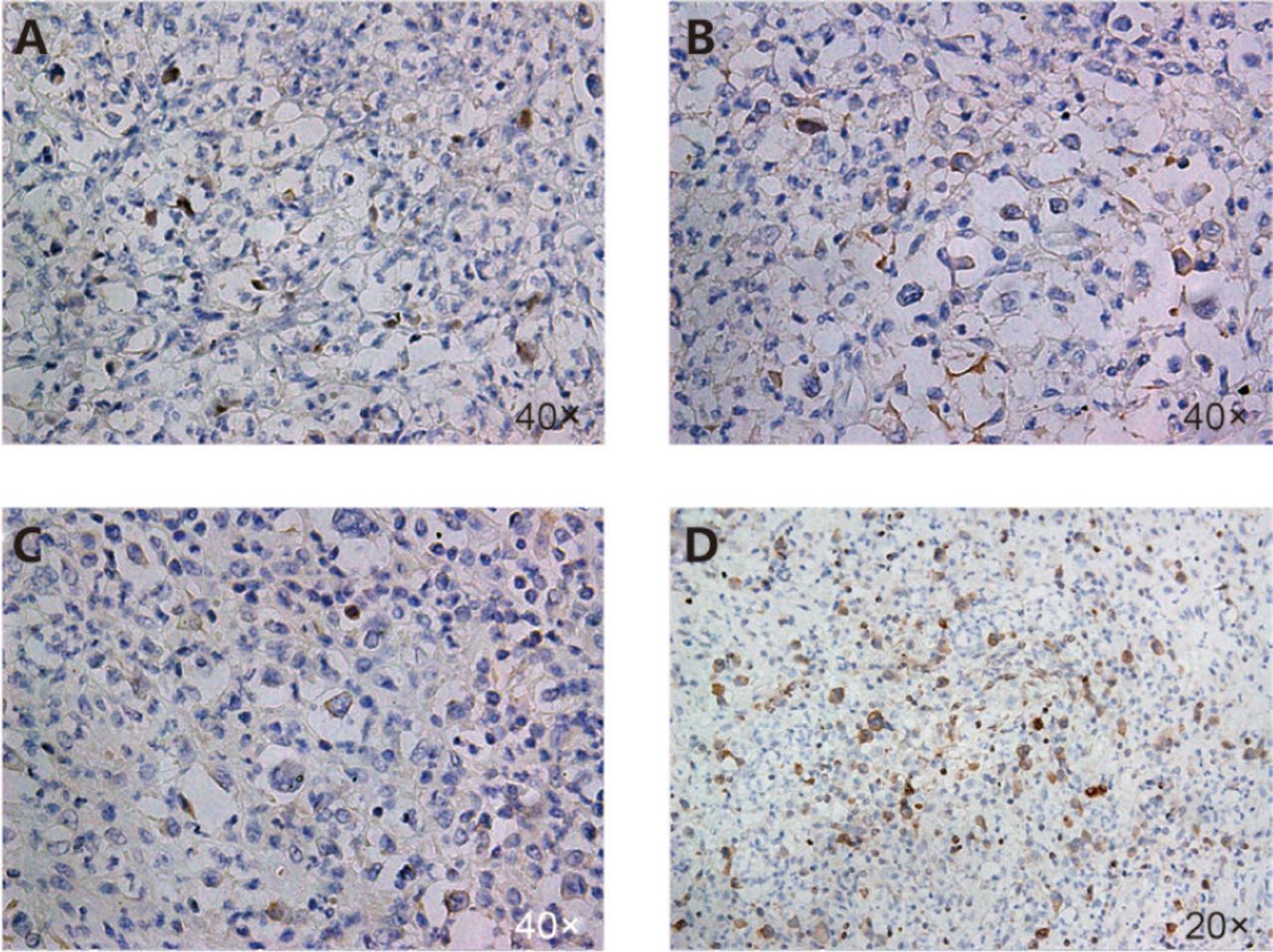
Immunohistochemically stained section of tissue obtained from the second case showing nodular sclerosis classical Hodgkin's lymphoma. The tissue was weakly positive for intranuclear staining (indicating the presence of ER) (A, B), hardly positive for PR (C), and BCL2 is visible (D).
The level of estrogen is high in gestational reproductive organs, and ER is overexpressed or activated in lymphoma cells. These data provide functional evidence suggesting that estrogen stimulates lymphoma in gonadal organs. Lymphoma can also occur in other organs, and estrogen also plays a role in tumors in non-gonadal organs, such as stomach, lung, kidney, and throat16. Thus, we speculate that estrogen may promote development of lymphoma.
In conclusion, the cases reported and the literature reviewed in this study suggested that hormonal changes in pregnancy are related to lymphoma growth. The four cases have shown that lymphomas, even indolent lymphomas, grow rapidly during pregnancy. Estrogen may accelerate lymphoma progression by inhibiting apoptosis and/or increasing growth. It is underscored that not only early biopsy and diagnosis but also the treatment with a reasonable combination of chemotherapy in the second or third trimester should be performed. However, termination of early pregnancy is preferred to prolong maternal survival and improve treatment outcomes. Furthermore, defining the roles of estrogen in lymphoma offers a high theoretical value and a great practical significance in effective prevention and treatment of lymphoma during pregnancy.
Footnotes
Conflict of interest statement No potential conflicts of interest are disclosed.
- Received April 10, 2016.
- Accepted June 13, 2016.
- Copyright: © 2016, Cancer Biology & Medicine
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC BY) 4.0, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.