

Abstract
Sarcoidosis is a benign systematic granulomatous disorder of unknown etiology and is associated with various malignancies. However, granulomatous and metastatic lymph node lesions are difficult to distinguish even when using precise and modern diagnostic methods, such as positron emission tomography. Thus, histological verification is the only method that can be used to accurately describe the nature of this disease. In this article, we report a case of non-luminal HER-2/neu-positive breast cancer in a patient without history of sarcoidosis and suspected to have metastatic disease.
keywords
Introduction
Sarcoidosis is a benign systemic granulomatous disorder of unknown etiology. Sarcoidosis-related granulomatous reaction of the immune system could be attributed to environmental factors. However, data supporting this hypothesis remain controversial1. Clinical features of this disease include the following nonspecific symptoms: cough, dyspnea, erythema nodosum, febrile arthritis, uveitis, and parotitis. Nevertheless, 50% of the patients are asymptomatic at the time of diagnosis. Sarcoidosis commonly targets hilar and mediastinal lymph nodes, which are found in more than 90% of the patients2. The diagnosis is established on the basis of compatible clinical and radiological findings and supported by histological evidence in one or more organs of noncaseating epithelioid cell granulomas in the absence of organisms or particles3. The correlation between sarcoidosis and malignancy remains unclear, despite that this topic has been increasingly investigated. In this article, we report a case of non-luminal HER-2/neu-positive breast cancer in a patient without history of sarcoidosis and initially suspected to have metastatic disease.
Case report
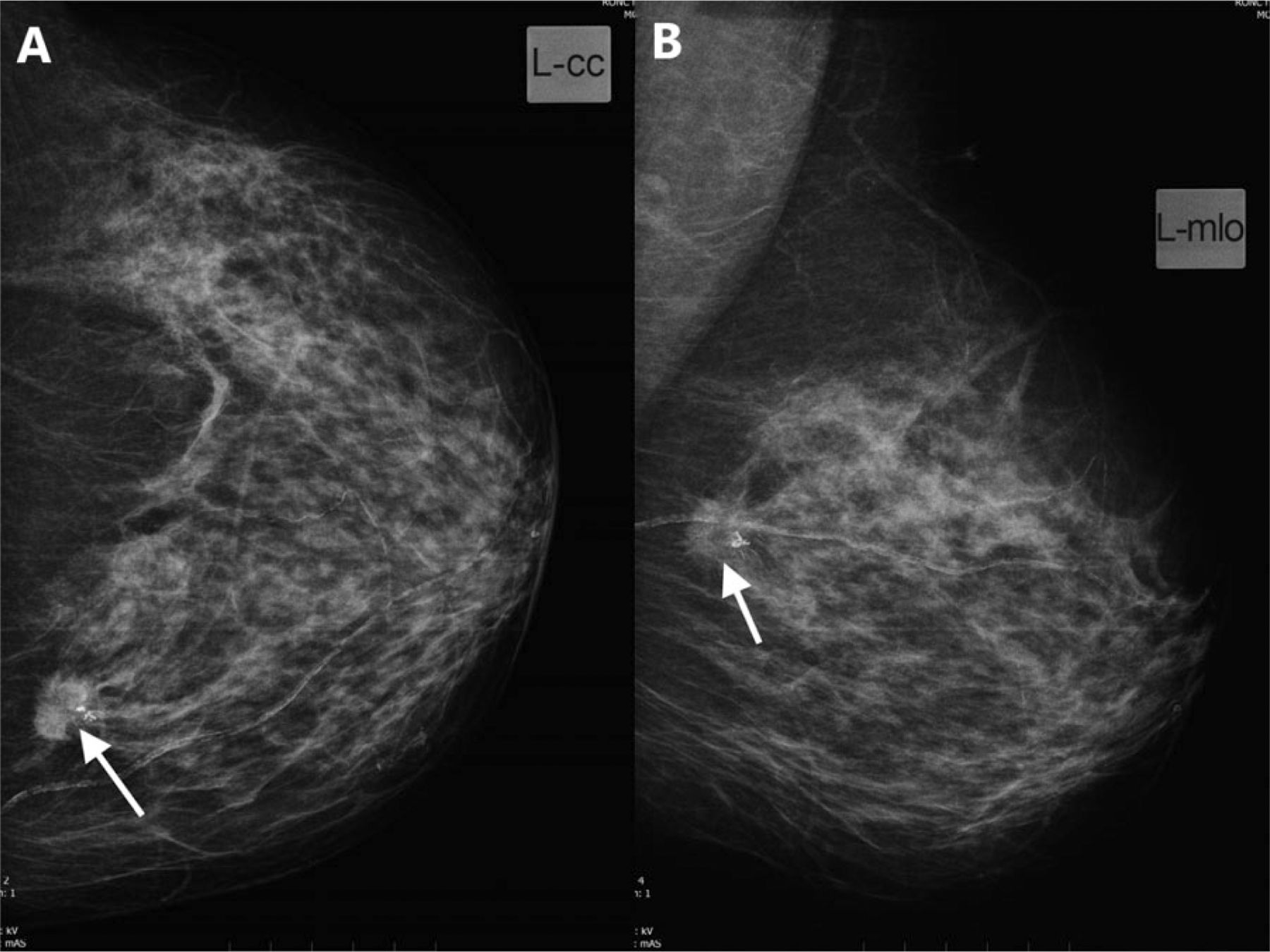
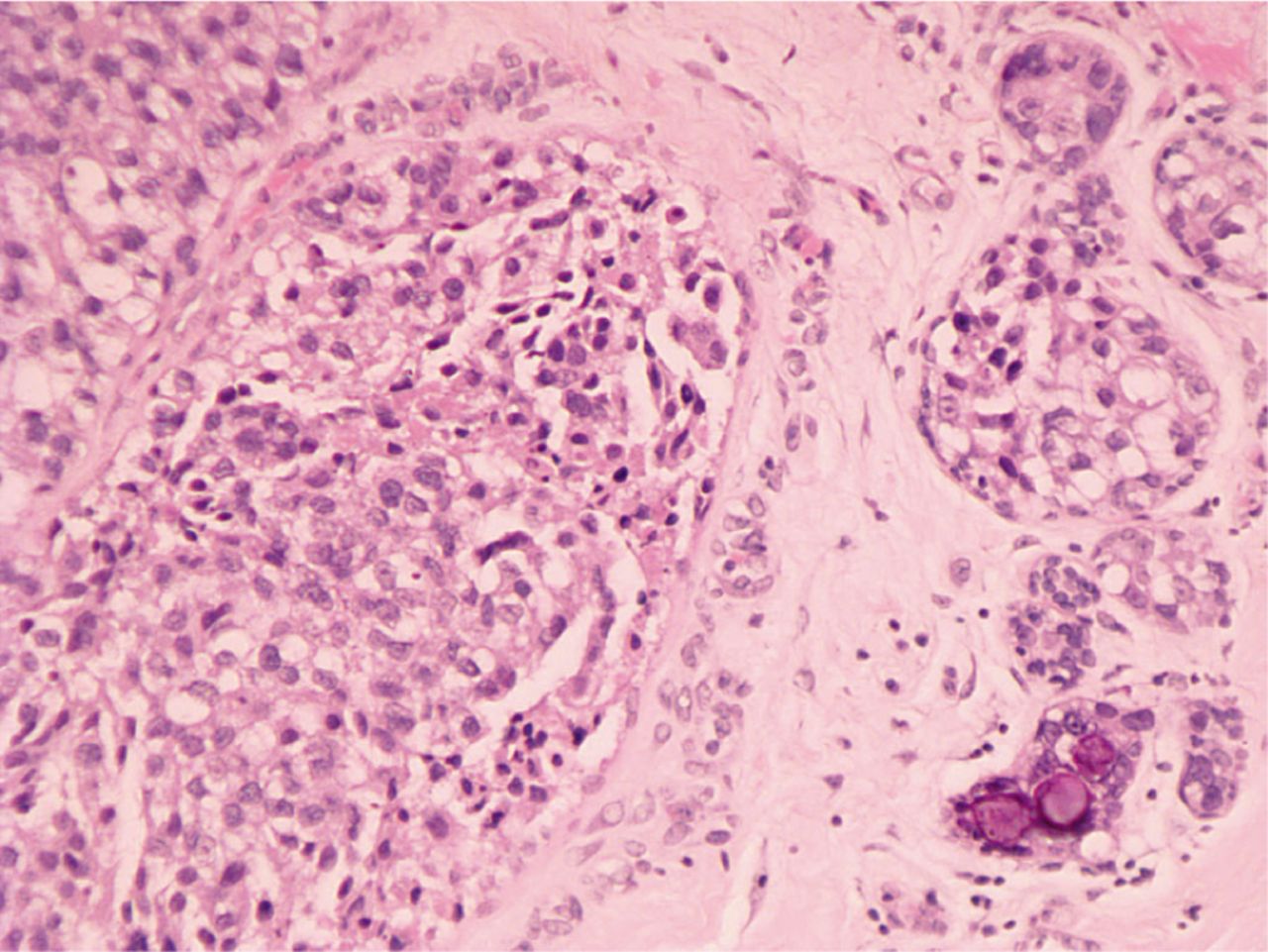
A 52-year-old woman was presented to our hospital. She noted a lump in her left breast during self-examination. The patient had no other complains about breasts. Clinical breast inspection and palpation revealed a nodular lump of tight, elastic consistency in the upper inner quadrant of the left breast. Mammography scan demonstrated a 19 mm × 18 mm mass on the border of the inner quadrants on the left breast (Figure 1). Ultrasound examination revealed enlarged lymph nodes in the left axilla (10 mm in diameter), left supraclavicular lymph node (18 mm × 10 mm), and multiple right enlarged supraclavicular lymph nodes, with a maximum size of 16 mm × 7 mm. Fine-needle aspiration cytology of the breast lump revealed atypical cells. Plain chest X-rays showed no abnormal findings (Figure 2). The suspected diagnosis was breast cancer at T1N3cM0. Excisional biopsy of the left supraclavicular lymph node was performed to verify the diagnosis and differentiate the nature of the lesion. Histological examination of the obtained material revealed no cancer but multiple epithelioid cell granulomas. Based on these results, lumpectomy with urgent histology of resection margins was selected for subsequent disease management. Urgent histodiagnosis revealed clear margins and demonstrated a lump in the breast, which was identified as infiltrative carcinoma. Prophylactic left axillary dissection was performed through a separate incision. Routine histological examination revealed infiltrative, moderately differentiated (G2) breast carcinoma with microcalcifications (Figure 3). Noncaseating epithelioid cell granulomas of sarcoidosis without tumor growth were found in 6 of 15 lymph nodes (Figure 4). The molecular type of breast cancer was identified as non-luminal HER-2/neu-positive through immunohistochemistry. Therefore, the post-operative diagnosis of the patient was left breast cancer (T1N0M0), with sarcoidosis of left axillary and right supraclavicular lymph nodes. At the time of writing this article, the patient had been undergoing radiation therapy and directed to immunologist for sarcoidosis management and follow-up.
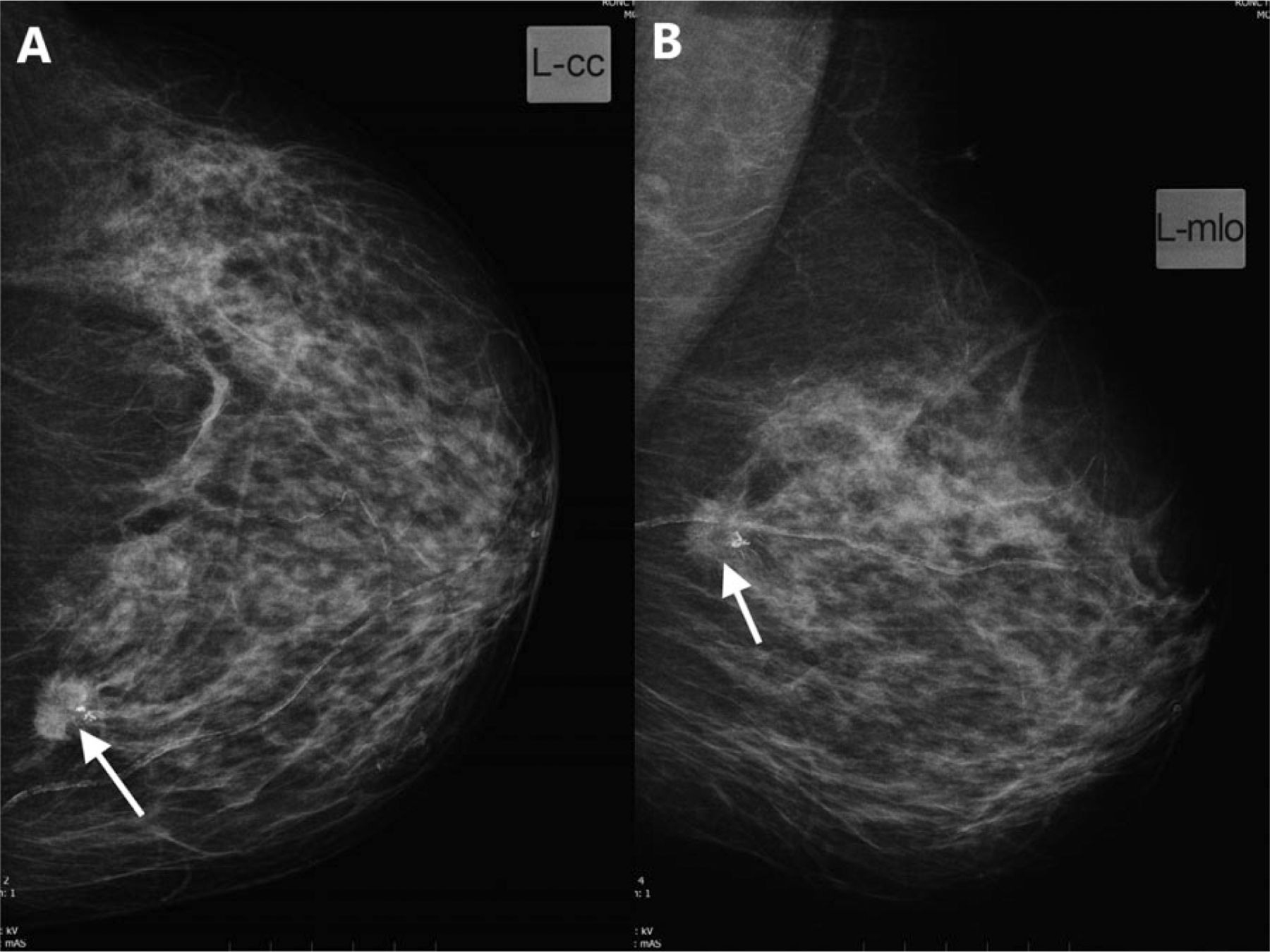
Mammography scan demonstrating a 19 mm × 18 mm mass on the border of the inner quadrants of the left breast (white arrow). (A) Craniocaudal. (B) Mediolateral oblique view.

Plain chest X-ray revealed no abnormal findings.

Infiltrative moderately differentiated (G2) breast carcinoma with microcalcifications (H&E staining, 200×).
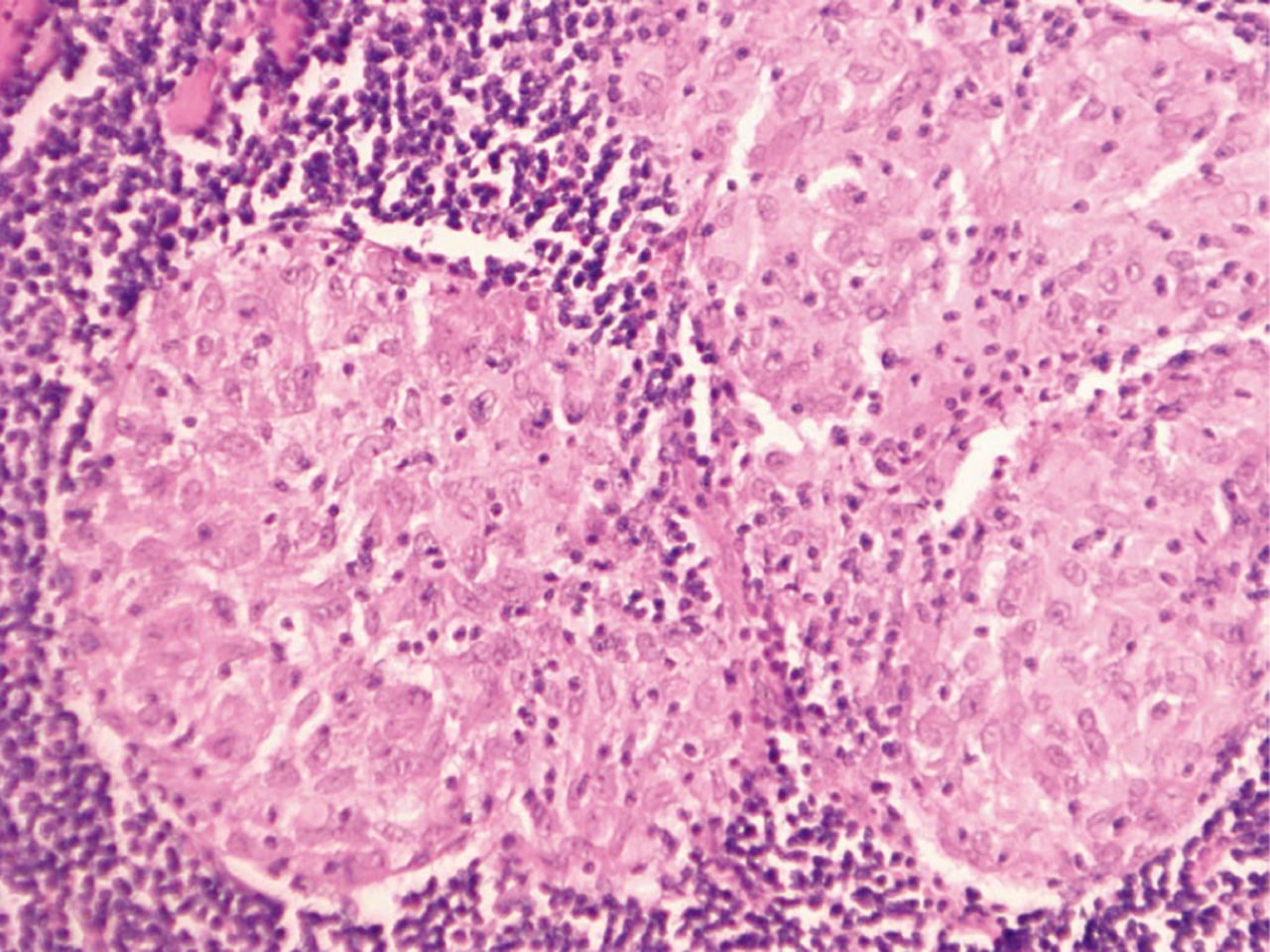
Lymph nodes with noncaseating epithelioid cell granulomas of sarcoidosis without tumor growth (H&E staining, 200×).
Discussion
The correlation between sarcoidosis and carcinogenesis remains unproven, although such relation has been described in numerous studies. Brincker and Wilbek4 first found this link in their study on 2544 sarcoidosis cases; the incidence rates of lymphomas and lung cancer were 11 and 3 fold higher, respectively, in patients with sarcoidosis than those in the population. The incidence rate of breast cancer is high among patients with sarcoidosis. Hunt et al.5 reported 21 cases of sarcoidosis developing after primary malignancies, including 10 cases after breast cancer. Butt et al.6 described 10 cases of breast cancer among 30 patients with sarcoidosis and malignancies. Blank et al.1 defined breast cancer, cervical cancer, and B-cell lymphoma as the most common malignancies in patients with sarcoidosis.
Oncologic diseases should be promptly and carefully diagnosed. Positron emission tomography (FDG-PET/CT scan) is one of the most advanced and precise diagnostic tools for such diseases. However, the application of this method in the assessment of regional and distant metastasis spread is limited7. In cases of simultaneous sarcoidosis and malignancies, the functions of FDG-PET/CT are further limited because tumor and granulomatous tissue both uptake fluorodeoxyglucose. Karam et al.8 identified that the maximal standardized uptake value (SUV) in patients with maligna- ncies is significantly higher than in patients with benign diseases. Nevertheless, in patients with granulomatous process, the maximal SUV is similar to that in patients with malignant diseases. Therefore, FDG-PET/CT scan may only be an additional diagnostic tool used to assess the extent of disease spread without differentiation between malignant and granulomatous disorders; this tool could also create diagnos- tic difficulties and misunderstandings in patients with such simultaneous comorbidities9,10. Only histological verification could accurately describe the nature of the disease.
This study reports a case of non-luminal HER-2/neu-positive breast cancer in a patient presenting non-caseating epithelioid cell granulomas of sarcoidosis after treatment and initially suspected to have metastatic disease. The diagnosis was established on the basis of clinical and radiological findings. A very recent retrospective study described the clinical biological and radiological characteristics of 12 patients presenting sarcoidosis associated with solid tumor; sarcoidosis frequently affects patients with breast cancer (32.3%) and thus must be considered in the differential diagnosis of the disease3. In the current study, a review of literature is also presented and included 61 other patients showing similar association between cancer and sarcoidosis.
This case report emphasizes the importance of differential diagnosis of lymph node involvement in cancer patients. Diagnosis of sarcoidosis denied that the presence of metastasis could lead to changes in the post-operative management of the patient. Although several epidemiological studies reported the association between cancer and sarcoidosis, further studies, including case reports, may represent an opportunity to obtain additional biological and clinical information to clarify the mechanisms underlying the association of cancer and sarcoidosis. Furthermore, the present case report highlights the importance of histological determination in lymph nodes for distinguishing metastasis from sarcoidosis.
Footnotes
Conflict of interest statement No potential conflicts of interest are disclosed.
- Received April 9, 2016.
- Accepted May 10, 2016.
- Copyright: © 2016, Cancer Biology & Medicine
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC BY) 4.0, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.