
Abstract
OBJECTIVE Interleukin-10 (IL-10) is a multifunctional cytokine with both immunosuppressive and antiangiogenic functions. Previous studies have reported that IL-10 levels are significantly elevated in patients with gastric cancer (GC). It has also been confirmed that interindividual variations in IL-10 production are genetically attributed to the polymorphisms of IL-10 gene. Therefore, this study was designed to investigate whether the polymorphisms of IL-10 gene were associated with susceptibility to GC in the Chinese population.
METHODS The serum levels of IL-10 were measured by radioimmunoassay. The single nucleotide polymorphisms (SNPs) at positions -1082A/G, -819T/C and -592A/C in the IL-10 gene promoter were analyzed using polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP).
RESULTS 220 patients with gastric cancer and 180 healthy controls were included in this study. The serum levels of IL-10 were significantly higher in GC patients than healthy controls (Z = -19.13, P < 0.001). Single SNP analysis showed that the -1082G allele, -1082AG and -819CC genotypes significantly increased in patients with GC (P = 0.029, 0.021, 0.039 respectively). In a logistic regression analysis adjusted for age and sex, the -1082AG genotype was associated with an odds ratio of 1.974 (95% CI, 1.14-3.391; P = 0.014), and the -819CC genotype with an odds ratio of 2.496 (95% CI, 1.222-5.102; P = 0.012) for GC. Furthermore, haplotype analysis revealed that at least five haplotypes (ATA, ACC, GCC, ACA and ATC) were existent in this population. Also that the GCC haplotype was associated with a significantly increased risk of GC as compared with the ATA haplotype (OR = 1.90; 95% CI, 1.11-3.27; P = 0.02).
CONCLUSION The results indicate that the gene haplotype of IL-10 may contribute to the susceptibility to GC in the Chinese population.
- interleukin-10
- polymorphism
- single nucleotide
- haplotypes
- stomach neoplasms
Introduction
Gastric cancer (GC), the second leading cause of death from cancer throughout the world, is particularly prevalent in certain countries, including China. It is generally accepted that Helicobacter pylori (H. pylori) infection has a close association with the development of GC. However, only a small portion (probably < 3%) of H. pylori-infected patients develop GC, indicating that additional factors must be involved in the disease process[1,2]. There is increasing evidence that many cytokines play an important role in the development of GC, such as tumor necrosis factor (TNF), Interleukin (IL)-6, IL-8 and IL-10. Increased levels of these cytokines have been reported in GC patients[3-6]. In addition, it is well known that promoter regions of cytokine genes contain polymorphisms that may directly influence the cytokines transcription or expression[7]. So these gene promoter polymorphisms may cause inter-individual differences in antitumor immune response and subsequently influence the susceptibility to GC through changing the production of cytokines.
IL-10 is a multifunctional cytokine with both immunosuppressive and antiangiogenic functions and may have both tumor-promoting and -inhibiting properties. Previous studies have demonstrated that the levels of IL-10 are elevated in patients with GC[6,8]. The gene encoding IL-10 is located on chromosome 1 at q31–32, and comprises 5 exons and 4 introns. It has been reported that there are 3 common SNPs at positions -1082A/G, -819T/C and -592A/C, which may influence the transcription of IL-10 messenger RNA and the expression of IL-10 in vitro and in vivo. In addition, the GCC haplotypes (defined by 3 SNPs at positions of -1082, -819 and -592) are associated with higher IL-10 expression compared with the ATA haplotypes[9,10]. Over the last 2 decades, cytokine polymorphisms are considered to play an important role in the pathogenesis of GC, and a number of case-control studies were conducted to investigate the association between IL-10 gene polymorphisms and GC risk in humans[11-17]. However, the findings of those studies tended to be confusing and, in fact, often contradictory. Thus it is still unclear whether the 3 IL-10-1082/-819/-592 polymorphisms were associated with susceptibility to GC in the Chinese population.
With this background information in mind, the present study was designed to investigate the effect of the -1082A/G, -819T/C and -592A/C common polymorphisms of the IL-10 gene on the susceptibility to GC by genotyping patients with GC in a Chinese population.
Materials and Methods
Clinical data
A total of 220 GC patients (study group) and 180 healthy controls (control group) were included in the study. The diagnosis of GC was established by endoscopic examination and confirmed by histopathology. The controls were recruited among relatives of health professionals and blood donors. They had no personal or family history of cancer or other serious illness. All patients and controls repeated the 14C-UBT test 2 times. None of the enrolled participants had ever been treated for H. pylori eradication. To minimize ethnic biases within the population studied, all enrolled subjects were from the Han Chinese ethnic group. Written informed consent was obtained from each participant or a close relative, and the research protocol was approved by the Ethical Committee of the hospital involved.
Determination of serum IL-10 levels
At 6 am on the first day after admission peripheral venous blood was collected from each participant, in a fasting state. The serum levels of IL-10 were determined by a radioimmunoassay using an Interleukin Radioimmunoassay Kit (Beijing Sino-UK institute of Biological Technology) according to the manufacturer’s instructions.
Genotyping
Using a Wizard Genomic DNA Purification kit (Promega), genomic DNA was extracted from EDTA-anticoagulanted peripheral blood leukocytes of each subject. The polymorphisms at positions -1082, -819 and -592 of IL-10 were analyzed by using polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) method.
IL-10-1082A/G genotyping
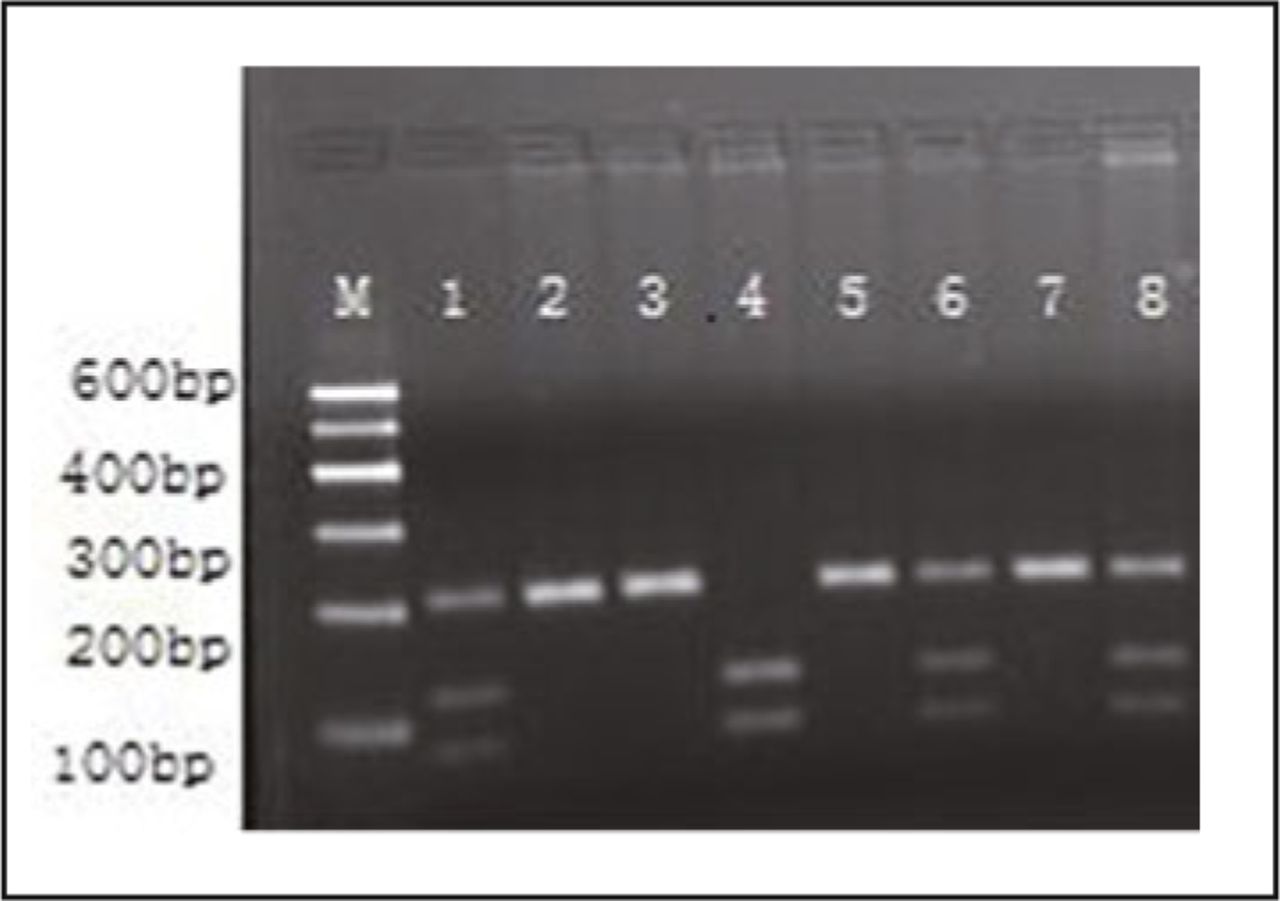
The primers were as follows: Forward, 5’-CCA AGA CAA CAC TAC TAA GGC TCCT TT-3’; reverse, 5’ -GCT TCT TAT ATG CTA GTC AGG TA-3’[18] (Shanghai Sangon Biological Engineering Technology & Services Co.). PCR condition consisted of 94°C 5 min, followed by 35 cycles of 94°C 30 s, 56°C 45 s and 72°C 1 min, with a final extension at 72°C for 10 min. PCR products were 377 bp and digested with 5 units of restriction enzyme EcoNI (New England Biolabs) at 37° C overnight. Digestion fragments of 280 bp + 97 bp for allele A or 253 bp + 97 bp + 27 bp for allele G, visualized by electrophoresis on a 3% agarose gel stained with 0.1% ethidium bromide (Fig. 1).

PCR-RFLP assay of −1082A/G IL-10 polymorphism. Lanes 1, 2, 3, 5, 6 and 7 are the homozygous AA genotype, showing A allele cut with EcoNI generating 280- and 97-bp fragments. Lanes 4 and 8 are the heterozygous AG genotype, with A allele cut with EcoNI generating 280- and 97-bp fragments, meanwhile, G allele cut with EcoNI generating 253-, 97- and 27-bp (not shown) fragments. Lane M is the marker.
IL-10-819T/C genotyping
The primers were as follows: Forward, 5’-TCA TTC TAT GTG CTG GAG ATG G-3’; reverse, 5’-TGG GGG AAG TGG GTA AGA GT-3’[19] (Shanghai Sangon Biological Engineering Technology & Services Co.). PCR condition consisted of 94°C 5 min, followed by 35 cycles of 94°C 30 s, 56°C 45 s and 72°C 1 min, with a final extension at 72°C for 10 min. PCR products were 209 bp and digested with 5 units of restriction enzyme Mae III (Roche) at 55°C for 1 h. Digestion fragments of 125 bp + 84 bp for allele C or 209 bp for allele T, visualized by electrophoresis on a 3% agarose gel stained with 0.1% ethidium bromide (Fig. 2).
PCR-RFLP assay of −819T/C IL-10 polymorphism. Lane 4 is the homozygous CC genotype, showing C allele cut with Mae III generating 125- and 84-bp fragments. Lanes 1, 6 and 8 are the heterozygous CT genotype, with C allele cut with Mae III generating 125- and 84-bp fragments, while T allele does not cut. Lanes 2, 3, 5 and 7 are the homozygous TT genotype, T allele does not cut, only 209-bp fragment. Lane M is the marker.
IL-10-592A/C Genotyping
The primers were as follows: Forward, 5’-GGT GAG CAC TAC CTG ACT AGC-3’; reverse: 5’-CCT AGG TCA CAG TGA CGT GG-3[19] (Shanghai Sangon Biological Engineering Technology & Services Co.). PCR condition consisted of 94°C 5 min, followed by 35 cycles of 94°C 30 s, 64°C 45 s and 72°C 1 min, with a final extension at 72°C for 10 min. PCR products were 412bp and digested with 5 units of restriction enzyme Rsa I (MBI Fermentas) at 37°C for 4 h. Digestion fragments of 176 bp + 236 bp for allele A or 412 bp for allele C, visualized by electrophoresis on a 3% agarose gel stained with 0.1% ethidium bromide (Fig. 3).

PCR-RFLP assay of −592A/C IL-10 polymorphism. Lanes 2, 4, 5 and 6 are the homozygous AA genotype, showing A allele cut with Rsa I generating 176- and 236-bp fragments. Lanes 3, 7 and 8 are the heterozygous AC genotype, with A allele cut with Rsa I generating 176- and 236-bp fragments; while C allele does not cut. Lane 1 is the homozygous CC genotype, C allele does not cut, only 412-bp fragment. Lane M is the marker.
Statistical analysis
The serum IL-10 levels were expressed as Mean ± SD and compared by the Mann-Whitney U test. A χ2 test and a 2-sample t-test were used to compare the demographic and clinical data between groups. A χ2 test was used to test the genotype distributions at each SNP locus with Hardy-Weinberg equilibrium. Genotype and allele frequencies were compared between study group and control group using the χ2 test and Fisher’s exact test when appropriate. Odds ratios (ORs) and 95% confidence intervals (CIs) for the associations of the IL-10 gene polymorphisms with the risk of GC were calculated by logistic regression analysis. Haplotypes and linkage disequilibrium (LD) were determined based on the expectation-maximization algorithm using the SNPStats program (available at http://bioinfo.iconcologia.net/SNPstats; Biostatistics and Bioinformatics Unit, Catalan Institute of Oncology, Barcelona, Spain). Statistical analyses were performed using the SPSS statistical software package (version 12.0). The P values were two-sided and P < 0.05 was considered statistically significant.
Results
Clinical characteristics of the study population
The characteristics of the participants enrolled in this study are shown in Table 1. There were no significant differences between the study group and control group for the mean age and gender distribution (P > 0.05). As seen in the table, there was no difference in the prevalence of H. pylori infection between study group and control group (P > 0.05).
Clinical characteristics of the patients with gastric cancer and control group.
Serum IL-10 levels in study group and control group
The serum levels of IL-10 in GC patients were significantly higher than those in healthy controls (72.47 ± 21.35 ng/mL vs. 36.82 ±15.88 ng/mL; Z = -19.13, P < 0.001).
The association between IL-10 gene polymorphisms and serum IL-10 levels
The IL-10-1082AG genotype was associated with higher IL-10 production as compared with the -1082AA genotype (Z = -17.24, P < 0.001). Similarly, the -819CC genotype was associated with higher IL-10 production as compared with the -819TT genotype (Z = -2.05, P = 0.041) (Fig. 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
The association between IL-10 gene polymorphisms and serum IL-10 levels.
The allele and genotype frequencies of IL-10 promoter
The allele and genotype frequencies of the IL-10 gene -1082A/G, -819T/C and -592A/C polymorphisms for all the studied variations are summarized in Table 2. Within each study group, the genotype distributions were consistent with those predicted by the Hardy-Weinberg equilibrium.
The genotype and allele frequencies of IL-10 polymorphism in patients with gastric cancer and control group.
A higher frequency of -1082G allele was observed in GC patients (P = 0.029). In addition, there were significant differences in the genotype frequencies of the IL-10 gene -1082A/G and -819T/C polymorphisms between GC patients and healthy controls (P = 0.021, 0.039 respectively). In a logistic regression analysis adjusted for age and sex, the -1082AG and -819CC genotypes were associated with an increased risk of GC (-1082AG OR = 1.974, 95% CI, 1.149-3.391, P = 0.014; -819CC OR = 2.496, 95% CI, 1.222-5.102, P = 0.012).
However, genotype and allele frequencies of the IL-10-592A/C polymorphisms in GC patients were not significantly different to those in healthy controls (P > 0.05).
Haplotype analysis of the IL-10 promoter
Haplotype analyses were performed and the possible 5 haplotype frequencies are shown in Table 3.
IL-10 gene haplotype distribution in the patients with gastric cancer and control group.
LD was observed between allele A at locus -1082 and allele T at locus -819 [D’ = 0.9989] and allele A at locus -1082 and allele A at locus-592 [D’ = 0.9989] and allele T at locus -819 and allele A at locus -592 [D’ = 0.9296]. Haplotype analysis revealed major ATA haplotype accounted for 62.0% and 66.1% of these five haplotypes in both GC patients and healthy controls, respectively. By haplotype analyses, we found that GCC haplotype was associated with a significantly increased risk of GC as compared with the ATA haplotype (OR = 1.90; 95% CI, 1.11-3.27; P = 0.02).
Discussion
In the present study, the IL-10 levels in 220 patients with GC and 180 healthy controls were detected; it was found that the serum levels of IL-10 in GC patients were significantly higher than those in healthy controls. Meanwhile, the association between the IL-10 gene polymorphisms and risk of GC was investigated in the study population. There were no significant differences in the distribution of the IL-10-592A/C polymorphisms between GC patients and healthy controls. However, the frequency of -1082G allele was increased in patients with GC. In addition, the presence of -1082AG and -819CC genotype was associated with an increased risk of GC in the study population. Furthermore, haplotype analysis revealed that GCC haplotype was associated with a significantly increased risk of GC as compared with the ATA haplotype.
IL-10 is a pleiotropic cytokine with both immunosuppressive and antiangiogenic functions and may have both tumor-promoting and -inhibiting properties. The elevated levels of IL-10 in GC patients have been reported. Zhang et al.[8] and Szaflarska et al.[6] reported that the levels of IL-10 in GC patients were significantly higher than those in healthy controls. However, the number of participants in those studies was relatively small. In the present study, researchers measured the IL-10 levels in 220 patients and 180 healthy controls and found that the serum levels of IL-10 in GC patients were significantly higher than those in healthy controls, which was consistent with previous studies. It may be explained by the knowledge that the anti-inflammatory characteristics of IL-10 can downregulate the host immune response, which, in turn, causes the development of GC. Furthermore, in this study, we also analyzed the effects of IL-10 gene polymorphisms on the levels of IL-10 in serum. In agreement with previous reports[9,10], we found that -1082AG genotype was associated with a higher IL-10 level as compared with the -1082AA genotype. In addition, we also found that the -819CC genotype was related to a higher IL-10 level as compared with the -819TT genotype, which has not been reported previously. However, due to the relatively large P value (P = 0.041) in our study, we couldn’t confirm that it was not a false-positive result. Therefore more studies about the effects of −819C/T polymorphisms on IL-10 production are needed.
A number of studies have reported the association between IL-10 gene polymorphims and GC. However, the findings of those studies were confusing and often contradictory. For example, El-Omar et al.[11] and Zambon et al.[12] reported that the IL-10-1082A/A, -819T/T or -592A/A genotype or the ATA haplotype of IL-10 polymorphisms was associated with an increased risk of H. pylori infection-related GC development. Deng et al.[13] reported that IL-10-1082A allele was associated with an increased risk of noncardia gastric cancer in his study population. However, other studies drew an opposite conclusion. Bai et al.[14] and Lu et al.[15] reported that IL-10-1082 promoter polymorphism was associated with an increased risk for GC in the Chinese population. But only a single SNP has been examined in those studies, making it difficult to exclude a role for other polymorphisms in the IL-10 gene concerned in the susceptibility to GC. Wu et al.[16] reported that the IL-10-1082G allele or the GCC haplotype, not the -1082A allele nor the ATA haplotype, was associated with a higher risk for GC development in her study population. A study conducted by M Sugimoto et al.[17] showed that the presence of IL-10-592C, -819C alleles and the GCC haplotype was associated with an increased risk for GC development in H. pylori-infected patients in Japan, however, that study suggested that the GCC haplotype was associated with low IL-10 production, which was contradictory to previous studies. In the present study, we investigated the IL-10 gene polymorphisms and found that the frequencies of -1082AG and -819CC genotypes were increased in GC patients. The logistic regression analysis suggested that the -1082AG and -819CC genotypes were associated with an increased risk of GC in the study population. Additionally, haplotype analysis revealed that GCC haplotype was associated with a significantly increased risk of gastric cancer as compared with the ATA haplotype in the study population. Considering that the association of IL-10 gene polymorphisms with the levels of IL-10 in serum, it is possible that the genetic variations of IL-10 can influence the susceptibility to GC through changing the production of IL-10.
It is noteworthy that, in the current study, the frequencies of the -1082AA and -1082AG were 81.8% and 18.3% respectively. No -1082GG genotype but at least five haplotypes (ATA, ACC, GCC, ACA and ATC) were found in the study population. These findings are significantly different from those reported by studies in Italian[20] and UK populations[21], but are similar to findings in previous studies from China[22]. It may be explained by the knowledge that a significant difference exists in the distribution of genotypes of IL-10 gene promoter in different ethnic groups[23].
In conclusion, the results of this study demonstrate that IL-10-1082AG, -819C/C genotype and the GCC haplotype have an association with increased risk of the development of gastric cancer in the study population. However, there were some limitations to this study. For example, the sample size was relatively small, and the inherent selection bias cannot be completely excluded in this study. Therefore further studies with larger sample sizes and an ethnically diverse cohort are needed to elucidate the genetic effects of the IL-10 polymorphisms on the risk of gastric cancer.
Conflict of interest statement
No potential conflicts of interest were disclosed.
- Received July 28, 2010.
- Accepted August 15, 2010.
- Copyright © 2010 by Tianjin Medical University Cancer Institute & Hospital and Springer