

Abstract
Objective: Oral squamous-cell carcinoma (OSCC) accounts for >90% of oral cancers affecting adults mostly between the fourth to seventh decades of life. The most common OSCC treatment is concomitant chemoradiotherapy (CCRT) having both loco-regional and distant control, but CCRT has acute and chronic toxic effects on adjacent normal tissue. This study aimed to determine the side effects of CCRT on the oral mucosa and to characterize the clinicopathology of oral lesions in patients with OSCC.
Methods: This descriptive, cross-sectional study was certified by the Ethical Review Committee (UHS/Education/126-12/2728) of the University of Health Sciences, Lahore, Pakistan. OSSC patients (n=81) with various histological subtypes, grades, and stages were recruited, and findings on their oral examination were recorded. These patients received 70, 90, and 119 Gy of radiotherapy dosages in combination with the chemotherapy drugs cisplatin and 5-fluorouracil. Data were analyzed using SPSS 20.0.
Results: The most common presentation of OSCC was a nonhealing ulcer (63%) involving tongue (55.6%). Clinical findings included mucositis (92.6%) and xerostomia of mild, moderate, and severe degrees in 11.1%, 46.9%, and 35.8% cases, respectively. Ulcers (87.7%), palpable lymph nodes (64.2%), limited mouth opening (64.2%) and fistula (40.7%) were also observed. In females, the association of radiotherapy dosage with limited mouth opening, xerostomia, and histological grading was statistically significant (P<0.05). The association of chemotherapy drugs with xerostomia (P=0.003) was also statistically significant.
Conclusions: CCRT induced mucositis, xerostomia, and trismus in patients with OSCC.
keywords
Introduction
Oral cancers are the eighth most common cancer worldwide, with the highest incidence in males1. According to the American Cancer Society, the incidence and prevalence of oral cancer is increasing in developed countries, and the mortality rate due to oral cancer is also rising in developing countries. In Southeast Asia, oral cancer is the second most common cancer and the second most common cause of death among males. In the same region, approximately one-third of worldwide cases and half of the deaths from oral cancer have been reported2.
More than 90% of oral cancers are squamous-cell carcinoma (SCC), which is frequently linked to heavy alcohol consumption and tobacco smoking1. Oral squamous-cell carcinoma (OSCC) is the most common tumor in Sri Lanka, Bhutan, India, Iran, Afghanistan, Maldives, Nepal, and Pakistan 3.
The Pakistan Medical Research Council has reported that oral cancer is the most common tumor in males, the second most common tumor in females after breast carcinoma, and the second most common tumor in both the genders4.
Radiation and chemotherapy are the most widely used cancer treatments. However, they are expensive and associated with many adverse reactions that increase patient morbidity and mortality5.
Acute reactions often occur in tissues with brisk cellular turnover rates, e.g., mucous membranes, which is responsible for the acute morbidity of the treatment. The damage may not become obvious in tissues with slow cellular turnover rates for months or years after therapy6,7. The effects of radiation therapy on normal tissues are divided into acute and chronic effects8. Oral complications include mucositis (stomatitis), xerostomia (dry mouth), loss of taste, infections (bacterial, fungal, or viral), dental caries, and osteoradionecrosis9. Oral mucositis significantly complicates cancer treatment due to weight loss, high risk of infection, pain, depression, dysphagia, and decreased quality of life14.
After the first week of conventional doses of radiation, erythema of oral mucosa obviously progresses in the next few weeks to mucositis, which ranges from small patches to ulcerated areas. Mucositis represents dead epithelial cells, inflammatory cells, and fibrin; it is sometimes superimposed by bacteria or yeast, and then patients complain of oral/throat pain during treatment8. Mucositis usually persists throughout treatment, peaks at the end of the irradiation period, and continues 1–3 weeks even after treatment cessation10. The frequency of mucositis with 5-florouracil chemotherapy agents is as high as 40%–70%. Frequencies of mucositis are considerably higher in patients receiving CCRT compared with those receiving radiation therapy alone11. Mucositis develops and resolves through four phases: initial inflammatory/vascular phase, epithelial phase, ulcerative/bacteriological phase, and healing phase12. With increased intensity of radiation and chemotherapy, adverse effects particularly oral mucositis also increase13. Oral mucositis significantly complicates cancer treatment due to weight loss, high risk of infection, pain, depression, dysphagia, and decreased quality of life14.
Loss of taste is a frequent complication of cancer treatment that begins early and progresses rapidly during the second week of treatment. Patients may complain of diminished acuity, strange sensation, or absolute lack of taste. Xerostomia is also a frequent problem that exacerbates taste loss. The improvement of taste is a slow process, and volume, composition, and production of saliva are also affected by radiation. Saliva production decreases to almost 50% after a week of treatment. Patients frequently complain ropy, tenacious, and thickened saliva, which may cause difficulty in speech, swallowing, and taste loss8.
Chronic complications of radiotherapy consist of mandible osteoradionecrosis, which is vert destructive. Soft-tissue fibrosis and ischemia are long-term effects of radiation therapy and may not be resolved at all. The main mechanism of osseous involvement is damage to the periosteal tissue and small vasculatures, the haversian canals. Fortunately, osteoradionecrosis is a rare complication, and the occurrence of osteoradionecrosis of maxilla is much less15–17. Trismus may result because of the fibrosis of masticatory muscles. Delayed wound healing can be a result of high-dose preoperative radiation. Without careful dental care during and after radiation therapy, patients are liable to accelerated caries and decay8.
Chemotherapy drugs damage tissues of rapidly dividing cells, i.e., skin, hair and nails. They also affect the mouth, bone marrow, and the lining of the digestive system. Side effects include mouth ulcers, change in taste, high risk of developing infections, tiredness, fatigue, diarrhea, constipation, easy bruising, and hair fall18. Similarly, toxic effects of CCRT are sore mouth, anemia, strange taste, increased risk of bleeding, nausea and vomiting, hair loss, lethargy, tingling and numbness in the fingers or toes, upset bowel (diarrhea/constipation), and tinnitus and high-frequency hearing loss19.
In the present study, OSCC patients during or at the end of CCRT subjected to primary surgical treatment were selected to determine the incidence of mucositis, xerostomia, and trismus.
Patients and methods
This descriptive study involved 81 histopathologically diagnosed OSCC patients from INMOL (Institute of Nuclear Medicine and Oncology Lahore) Hospital, Lahore, Pakistan who were on concomitant chemo-radiotherapy. After obtaining written informed consent, details of each patient (age, gender, addictive habits, site of tumor, clinical stage, and histologic grade) were recorded.
These patients underwent CCRT, with five fractions in five days per week to total radiotherapy dosages of 70, 90, and 119 Gy accordingly. The chemotherapy drugs cisplatin and 5-fluorouracil were given in 4, 6, and 8 cycles depending on the stage of tumor and nutritional status of patient. Adverse effects of CCRT were noted. Oral mucositis was categorized according to EORTC/RTOG criteria ( Table 1)20.
Oral mucositis scale according to EORTC/ RTOG
For the severity of xerostomia, the CTCAE grading scale (version 3.0) was used21,22. Xerostomia was classified as grade mild, moderate, and severe (Table 2).
Clinical grading of xerostomia
A mean RTOG/EORTC score was calculated from the observations of two experts and then compared with the patients’ reported scores. Each patient was asked to complete a patient-reported xerostomia questionnaire comprising eight items (Table 3) that rated symptoms on an 11-point ordinal Likert scale from 0 to 10, with higher scores representing discomfort due to greater dryness. Each point score was added, and the total was changed linearly to generate the final score varying from 0 to 100, with higher scores representing greater levels of xerostomia (Table 1)23.
Xerostomia questionnaire
Trismus was measured as follows:
In dentulous patients, distance was calculated between incisal edges of mandibular and maxillary central incisors.
In edentulous patients, distance was calculated between mandibular and maxillary alveolar ridges24.
All data were entered and analyzed using SPSS 20.0. Chi-squared test was used to determine statistical association among the study variables. A P value ≤0.05 was considered as statistically significant. Regarding the ethics of medical research in humans, authors observed the declaration of World Medical Association in Helsinki (2008). This study was also approved by the Ethical Review Committee of the University of Health Sciences (UHS), Lahore, Pakistan.
Results
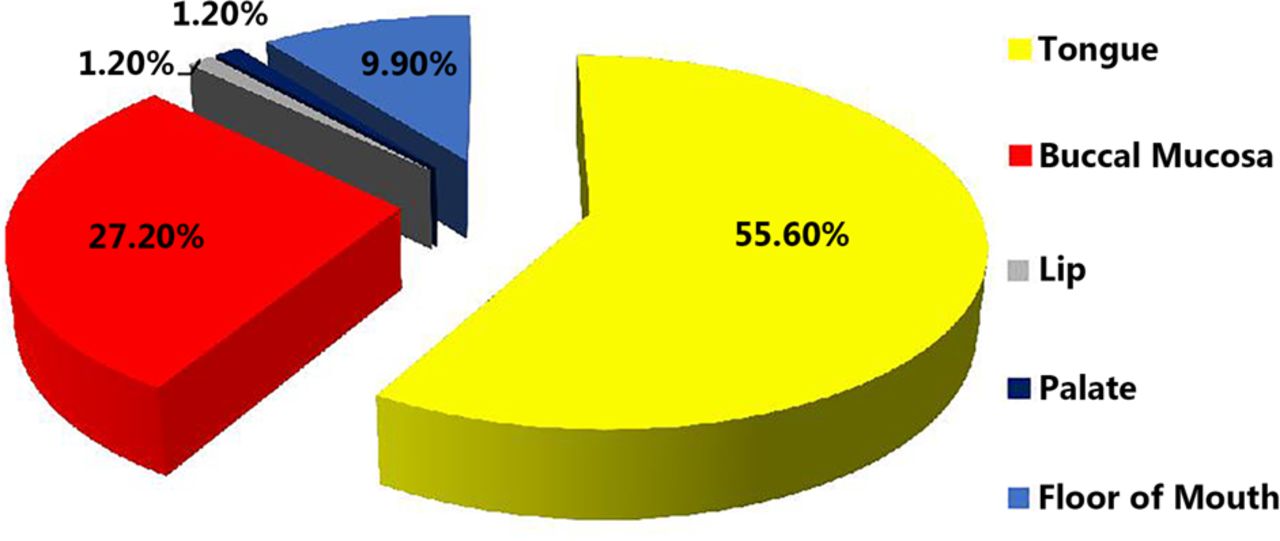
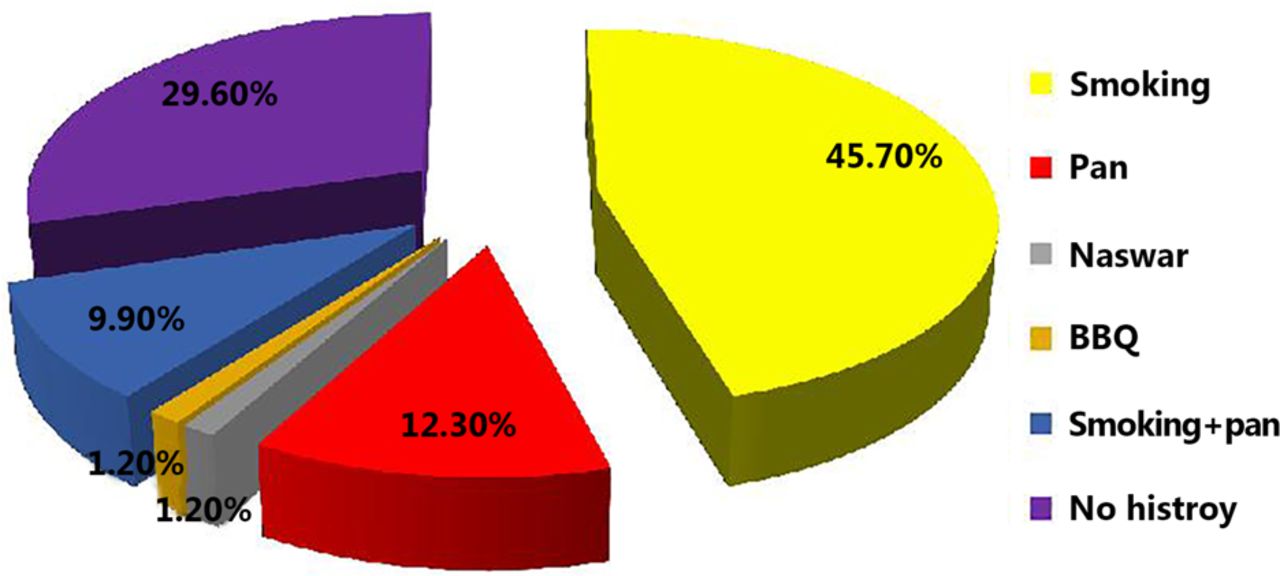
The age of OSCC patients was between 46–55 years, with a mean SD of 53.5±14.1 years; the male-to-female ratio was 1.4:1 (64.2% males and 35.8% females) (Figure 1). The most common OSCC presentation was a nonhealing ulcer (63%); the tumor sites were tongue (55.6%), buccal mucosa (27.2%), floor of mouth (9.9%), retromolar area (4.9%), and lip and palate (1.2%) (Figure 2). The history of smoking and pan chewing was 45.7% and 12.3%, respectively, whereas 29.6% of patients were without any history of addiction (Figure 3).
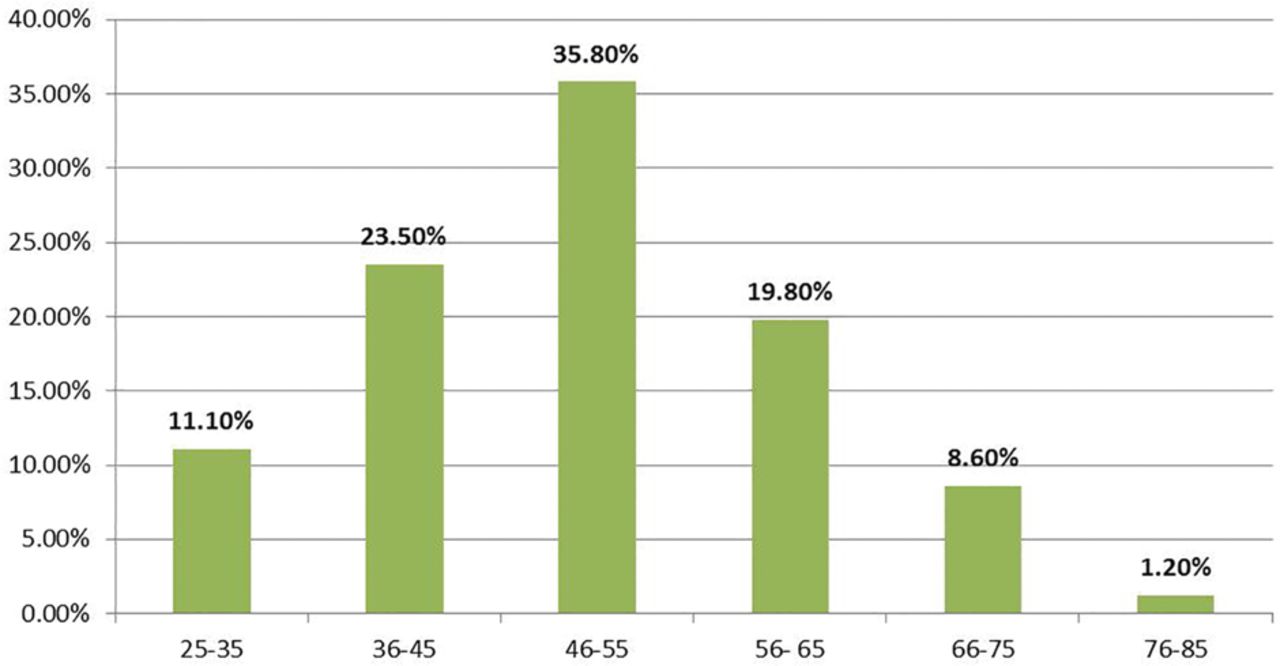
Incidence of OSCC in different age groups.
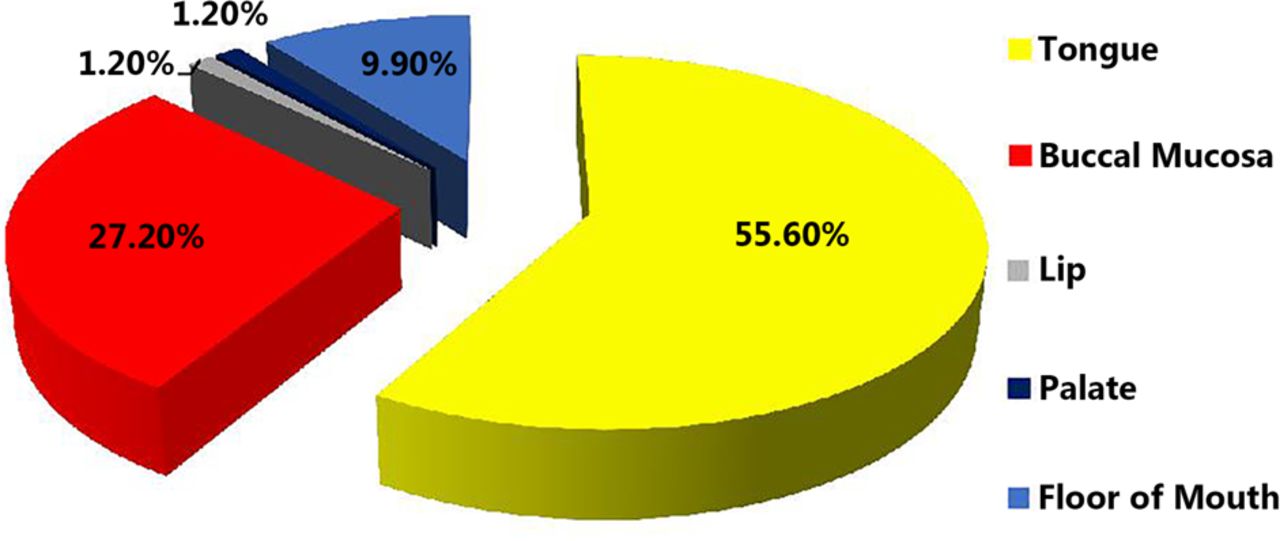
The site distribution of OSCC.
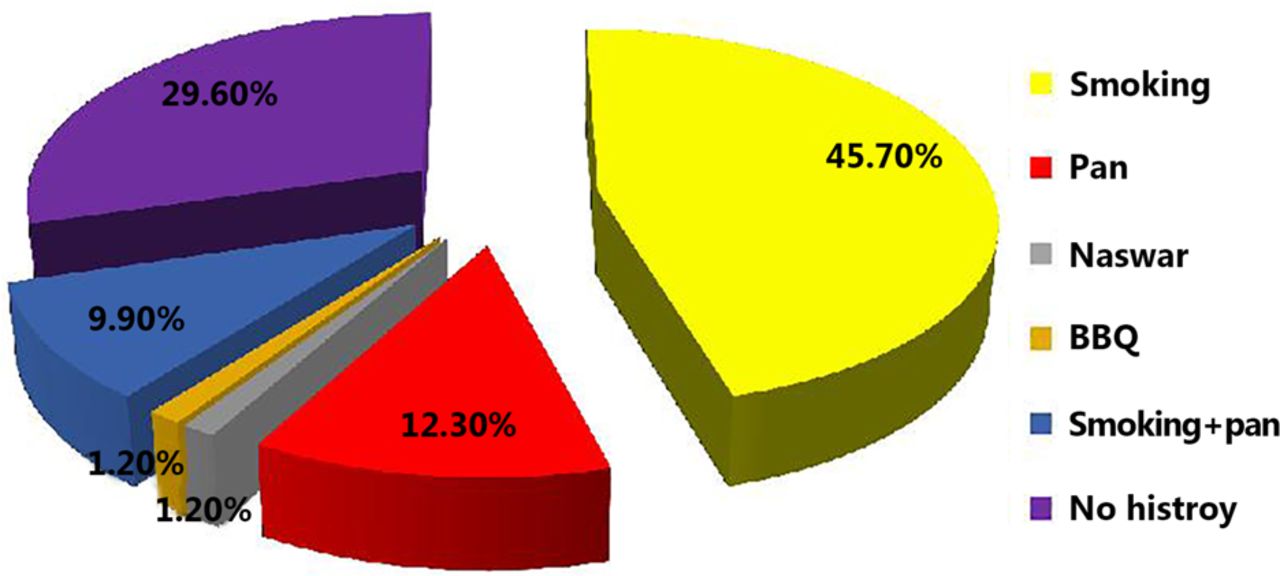
Addictive habits in OSCC patients.
Well, moderately, and poorly differentiated tumors were observed in 29.6%, 51.96%, and 14.8%, respectively. Regarding clinical staging of tumor, T4 stage was observed in the majority (57%), followed by T3 (28.4%), T2 (12.3%), and T1 (2.5%). Significant association was observed between the site of tumor and gender (P=0.036), habits of patients (P=0.018), gross appearance of tumor (P=0.001), and histological grading of tumors (P=0.024). A significant association was observed between age and clinical stage of tumors (P=0.035).
Associated complications included mucositis (92.6%) (Figure 4), xerostomia (mild, 11.1%; moderate, 46.9%; and severe, 35.8%), and fungal infection (60.5%). Limited mouth opening, palpable lymph nodes and fistula (Figure 5) were present in 64.2%, 64.2%, and 40.7%, respectively. A significant association was observed between dosage of radiotherapy and limited mouth opening, xerostomia (Figure 6), and histological grading. Similarly, a significant association was observed between chemotherapy drugs and xerostomia (P=0.003).

A 45-year-old female with no history of addiction, presented with OSCC of tongue. At the end of CCRT grade 4 mucositis was observed with sever xerostomia and poor oral hygiene as well as decayed and carious teeth.

A patient presented with OSCC of tongue and at the end of CCRT, a fistula was noted on the right lower border of the mandible.

A patient presented with OSCC of the posterior lateral border of tongue. At the end of CCRT, the patient complained about the thick, ropy saliva with grade 3 mucositis and loss of taste sensation as there was loss of papilla from the tongue surface.
Discussion
Most of the clinical features observed in patients with OSCC in this study were in accordance with earlier studies. Oral cancer mostly occurs in elderly people. The frequency of oral cancers increases with increased age25. The majority of studies reported OSCC in males, consistent with the findings of the current study, i.e., high incidence in the fifth to seventh decades of life26–28. The incidence of oral cancers has been recently noted at a younger age, and the same has been observed in the present study 28,29. Approximately 17% of patients were under 40 years of age30 or somewhere in the fourth decade of life31.
Tongue was the most commonly affected intraoral site in the present study, consistent with previous reports also suggesting the predilection of tongue for OSCC development32,33. However, diverse results have been reported, such as the high proportion of OSCC on the floor of mouth, proceeded by the tongue34,35. The intraoral spread of OSCC may be associated with the cultural and geographic differences in addictive habits of individuals, e.g., smokeless tobacco chewing in the subcontinent. The most common site of OSCC in these areas is buccal mucosa36.
OSCC treatment includes surgery, radiation therapy, chemotherapy, and CCRT depending on a patient’s risk factors, such as stage of cancer, age, immune status, and presence of comorbidities37. Chemotherapy is the choice for advanced tumor stages, tumors with no option of resection, and patients unsuitable for surgery, etc.33 In the current study, most patients presented with advanced tumor stage, i.e., T4. The chief goal of chemotherapy is to eliminate systemic micrometastasis, and the goal of administrating chemotherapy plus radiation concurrently is to develop regional and systemic control of tumor38. Currently, CCRT is the most excellent therapy for patients with regionally advanced solid tumors because it improves their survival rates and loco-regional control with organ protection39.
Radiation therapy and chemotherapy have severe side effects that decrease a patient’s quality of life40. Given that both radiotherapy and chemotherapy are used to treat locally advanced oral cavity tumors, the incidence of toxicities also increases.
In the present study, mucositis was observed in most patients during CCRT. International studies on mucositis and CCRT toxicity are in accordance with the present study. An increased incidence of mucositis has been reported with increased intensity of chemotherapy and radiotherapy, and in some cases, they appear as a “wave-like” pattern throughout the irradiation period41. Trotti et al.42 observed grade ≥3 mucositis in 20%–30% of patients treated with radiation therapy alone versus 40%–90% of patients treated with radiation plus concurrent chemotherapy. Sonis et al.43 reported that 64% of radiotherapy patients and 78% of chemotherapy patients had clinically visible mucositis. Apparently, the incidence of mucositis with radiotherapy is lower, but when chemotherapy is added to radiotherapy, the incidence and severity of mucositis increases. To prevent this complication of CCRT, patients are advised to maintain proper oral hygiene and dental care. Current clinical management of oral mucositis is mainly focused on palliative measures, such as nutritional support, maintenance of good oral hygiene, and pain management.
A severe complication of radiation therapy for head and neck tumors is radiation-induced xerostomia, which frequently occurs at the initial stage of treatment and strongly influences a patient’s everyday living44. The injury advances and becomes irreversible with increased radiation contact dose to the salivary glands 45–47. The association between dosage of CCRT and xerostomia is significant45,48–50, consistent with the present study.
Patients receiving radiation alone or on radio-chemotherapy have a considerably higher risk for trismus51,52. The present study observed a significant association between dosage of radiotherapy and trismus. With increased dose of radiotherapy, the frequency of trismus also increases. This finding agreed with that of Teguh et al.53, who reported that radiation-induced trismus varied with radiation dose, fraction of radiation, treatment technique, and overall time of treatment.
Conclusions
Frequent problems of patients with oral cancer on CCRT included mucositis, xerostomia, trismus, and difficulty in drinking and eating. All these toxicities were significantly associated with CCRT dose. Pretreatment measures should be taken to lessen these complications so that the patient’s nutritional status would not be compromised and the patient’s quality of life would not be affected.
Acknowledgements
All authors acknowledge the support extended by the staff of the Morbid Anatomy and Histopathology, UHS, Lahore and INMOL Hospital, Lahore.
Footnotes
↵*These authors have contributed equally to this work
Conflict of interest statement No potential conflicts of interest are disclosed.
- Received November 28, 2016.
- Accepted December 23, 2016.
- Copyright: © 2017, Cancer Biology & Medicine
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC BY) 4.0, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}