

Abstract
Breast metastasis from extra-mammary malignancy is rare. An incidence of 0.4% to 1.3% has been reported in literature. The primary malignancies that most commonly metastasize to the breast are leukemia, lymphoma, and malignant melanoma. In this report, two cases of pulmonary metastasis to the breast were presented. A 40-year-old female manifested a right breast mass of 2-month duration. After physical examination was performed, a poorly defined mass was noted in the upper outer quadrant of the right breast. Another 49-year-old female manifested right breast mass of 5-day duration. A poorly defined mass was noted in the lower inner quadrant of the right breast. Mammography results also revealed breast cancer. The patients underwent local excision. After histological and immunohistochemical analyses were conducted, a primary lung carcinoma that metastasized to the breast was diagnosed. An accurate differentiation of metastasis to the breast from primary breast cancer is very important because the treatment and prognosis of the two differ significantly.
keywords
Introduction
Primary breast cancer is one of the most common malignancies in adult females, in which metastases to the breast represent approximately 0.4% to 1.3% of malignant tumors in the breast in a clinical series1–4. Despite its rarity, metastatic breast disease is a significant diagnostic clinical problem because its treatment largely differs from that of primary breast cancer. In 1907, Sitzentfrey5 firstly published a case of ovarian carcinoma that metastasized to the breast. Thus far, various malignancies, including hematological malignancies, malignant melanoma, lung tumors, renal cell carcinoma, ovarian tumors, thyroid carcinomas, and small bowel carcinoids, have commonly metastasized to the breast2,4–8. The lung is one of the most common cancer sites in terms of incidence and mortality; however, cases of pulmonary carcinomas metastasizing to the breast have also been published (Table 1)9–24.
Breast metastasis from lung cancer: review of the literature (2003-2013)
Some cases presented breast metastasis from lung tumors. However, no detailed histological classification has been provided. In this report, two patients with breast metastases from pulmonary adenocarcinoma were presented. To our knowledge, this article is the first to report lung cancer cells as single lesions infiltrating into bilateral breast parenchymal tissues. We also performed a differential diagnosis by using a panel of immunohistochemical markers. Written informed consent was obtained from each patient for publication of this case report and accompanying images.
Case one
A 40-year-old non-smoking nurse was presented to the Tianjin Medical University Cancer Institute and Hospital with a right breast mass of 2-month duration. Physical examination results revealed a mass in the upper outer field of her right breast. The mass was hard and fixed. The skin of her breast was normal. Corresponding superficial lymph nodes were not enlarged. Mammography results revealed right breast cancer. Calcification was not observed. Enhanced chest computed tomography (CT) showed a cavitary mass in the posterior basal segment of the right lower lobe, metastatic nodules in bilateral lungs, and metastatic lymph nodes in the mediastinum and hilum of the right lung; a nodule in the upper outer quadrant of the left breast near the anterior axilla and multiple liver masses were also observed. Magnetic resonance imaging results indicated a nodule in the upper outer quadrant of the left breast near the anterior axilla, suggesting malignancy. Bilateral local excision was performed to remove the rapidly growing breast lesion. Our patient received chemotherapy of paclitaxel and cisplatin and lived for 7 months.
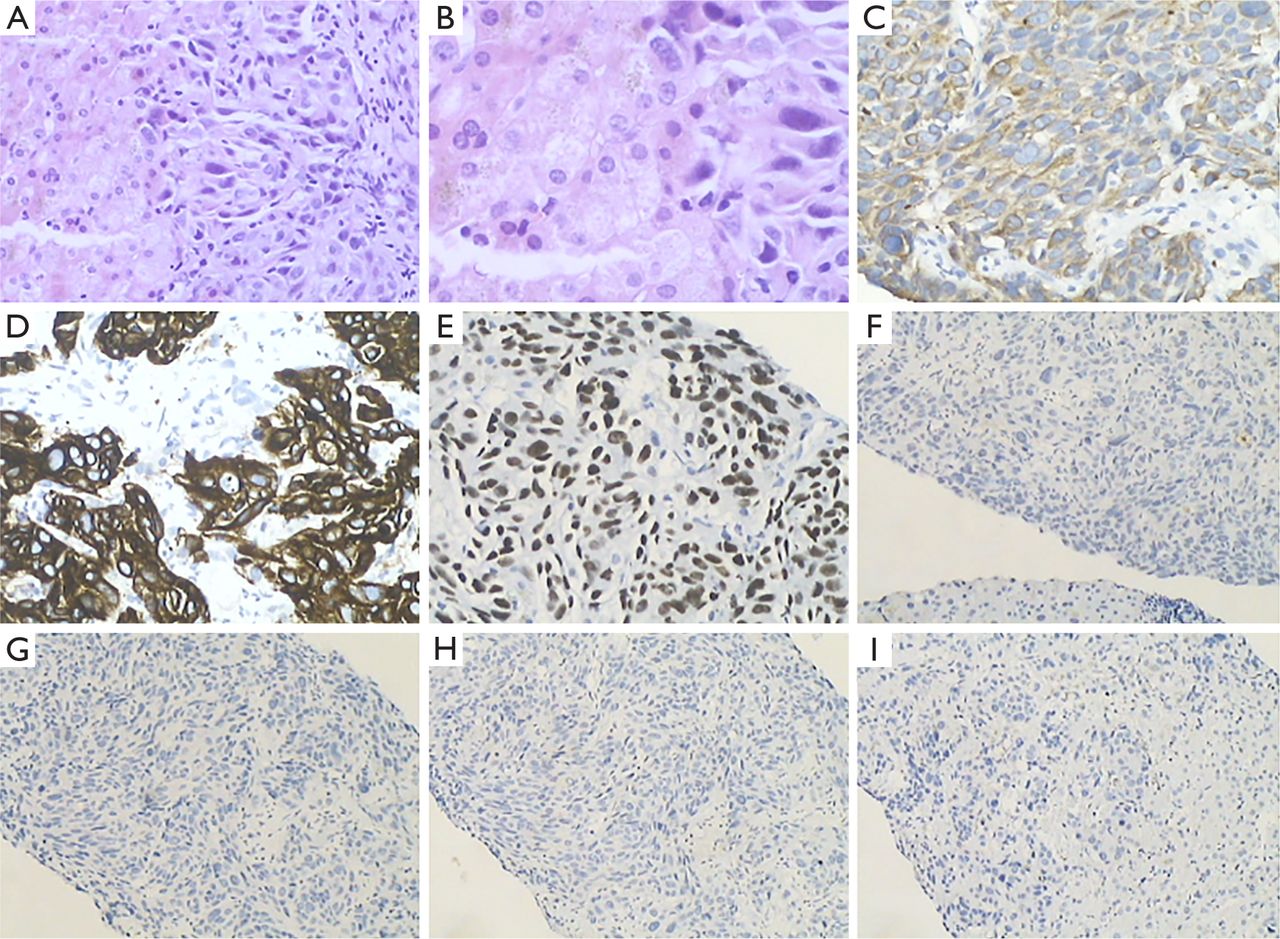
Hematoxylin and eosin (H&E)-stained paraffin sections of the breast specimen revealed spindle cell carcinoma. These poorly differentiated tumors were composed of large crowded clusters of cells with moderate to abundant cytoplasm; these tumors also displayed an infiltrative growth pattern. Furthermore, these tumors consisted of densely and solid nests of spindle cells separated by delicate fibrovascular stroma. In some tumors, nuclear streaming occurred. Our differential diagnosis included primary breast carcinoma and metastatic carcinoma from the lungs. The tumor cells demonstrated immunoreactivity for CK7, CK8, thyroid transcription factor-1 (TTF1), neuron-specific enolase (NSE), Syn, CgA, and SOX-2. The neoplastic cells lacked expressions of smooth muscle actin (SMA), p63, calponin, p40, gross cystic disease fluid protein-15 (GCDFP-15), mammaglobin (MG), CA15-3, estrogen receptor (ER), progesterone receptor (PR), c-erb-2, CK 5/6 and CD56. The expressions of Ki67 and p53 showed strong nuclear staining in 50% and 85% of the tumor cells, respectively. No evidence of in situ carcinoma was observed (Figure 1). Spindle cell neuroendocrine carcinoma metastasized from the lungs was diagnosed based on histological and immunohistochemical staining patterns (Figure 2); this result is consistent with contralateral breast tumor diagnosis.

(A) Specimen of the left breast biopsy. Tumor edge is ill-defined and lacks sharp circumscription. Tumor is hard upon palpation. Cut surface is gray white and gray red (0.7 cm × 0.6 cm × 0.5 cm). (B) Spindle cell carcinoma (H&E staining ×100). (C) TTF-1 positive (IHC staining ×100). (D) NSE positive (IHC staining ×100). (E) Syn positive (IHC staining ×100). (F) CgA positive (IHC staining ×100). (G) GCDFP-15 negative (IHC staining ×100). (H) MG negative (IHC staining ×100). (I) p63 negative (IHC staining ×100).
Differential diagnosis of case 1.
CT also showed multiple liver masses. Thus, we performed hepatic core needle biopsy. H&E-stained paraffin sections of the hepatic core needle biopsy specimen revealed carcinoma. The tumor cells demonstrated immunoreactivity for CK7, CK19 and TTF1. The neoplastic cells lacked expression of GCDFP-15, ER, PR, c-erb-2, CK20 and CD56 (Figure 3). Lung carcinoma metastasis was diagnosed based on histological and immunohistochemical staining patterns.
(A) Liver biopsy, carcinoma (H&E staining ×200); (B) Carcinoma. (H&E staining ×400); (C) CK7 positive (IHC staining ×200); (D) CK19 positive (IHC staining ×200); (E) TTF1 positive (IHC staining ×200); (F) GCDFP-15 negative (IHC staining ×100); (G) ER negative (IHC staining ×100); (H) PR negative (IHC staining ×100); (I) CK20 negative (IHC staining ×100).
Case two
A 49-year-old non-smoking housewife was presented to the Tianjin Medical University Cancer Institute and Hospital with a right breast mass of 5-day duration. Physical examination results revealed a mass in the lower inner field of her right breast. The mass was hard and fixed. The skin of her breast was normal. Corresponding superficial lymph nodes were not enlarged. Enhanced chest CT showed a right breast mass, a nodule in the right upper lung, and metastatic lymph nodes in the mediastinum and right collarbone. Right local excision was performed to remove the rapidly growing breast lesion. The patient initiatively abandoned chemotherapy and lived for 8 months.
The H&E-stained paraffin sections of the breast specimen revealed carcinoma. The tumors were composed of densely packed hyperchromatic cells with scant cytoplasm and displayed an infiltrative growth pattern. Crush artifact and nuclear streaming occurred. Our differential diagnosis included primary breast carcinoma and metastatic carcinoma from the lungs. The tumor cells demonstrated immunoreactivity for TTF-1, NSE and CD56. The neoplastic cells lacked expression of MG, CA15-3, ER, PR, c-erb-2, EGFR, Syn, CgA and LCA (Figure 4). The expression of Ki67 and p53 showed strong nuclear staining in 60% and 80% of the tumor cells, respectively. No evidence of in situ carcinoma was observed. Small cell lung carcinoma metastasis was diagnosed based on histological and immunohistochemical staining patterns (Figure 5).

(A) Specimen of the right breast biopsy. Tumor edge is ill-defined and lacks sharp circumscription. Tumor is hard upon palpation. Cut surface is gray white (3.2 cm × 3.0 cm × 2.7 cm). (B) Small cell carcinoma (H&E staining ×40). (C) Small cell carcinoma (H&E staining ×100). (D) TTF-1 positive (IHC staining ×100). (E) CD56 positive (IHC staining ×200). (F) CA153 negative (IHC staining×100). (G) ER negative (IHC staining ×100). (H) PR negative (IHC staining ×100). (I) c-erb-2 negative (IHC staining ×100).

Differential diagnosis of case 2.
Discussion
Patients with breast metastasis from pulmonary adenocarcinoma usually present a rapidly growing, painless, firm, well-circumscribed, and palpable mass with a predilection to the upper outer quadrant1,6,7,12. Unlike primary tumors, metastases do not generally demonstrate skin or nipple retraction despite their superficial location4,12. Distinguishing breast metastasis from primary mammary adenocarcinoma based on mammographic findings may be very difficult because of the wide range of imaging manifestations of metastatic lesions. Thus, metastasis can mimic a primary malignancy or even a benign breast tumor3,4,8. Mammography most commonly shows a well-defined rounded mass; however, multiple well-circumscribed lesions with smooth margins may also be presented2,8,20. Calcification is rare in breast metastases compared with metastases from serous papillary carcinoma of the ovary8,20,23.
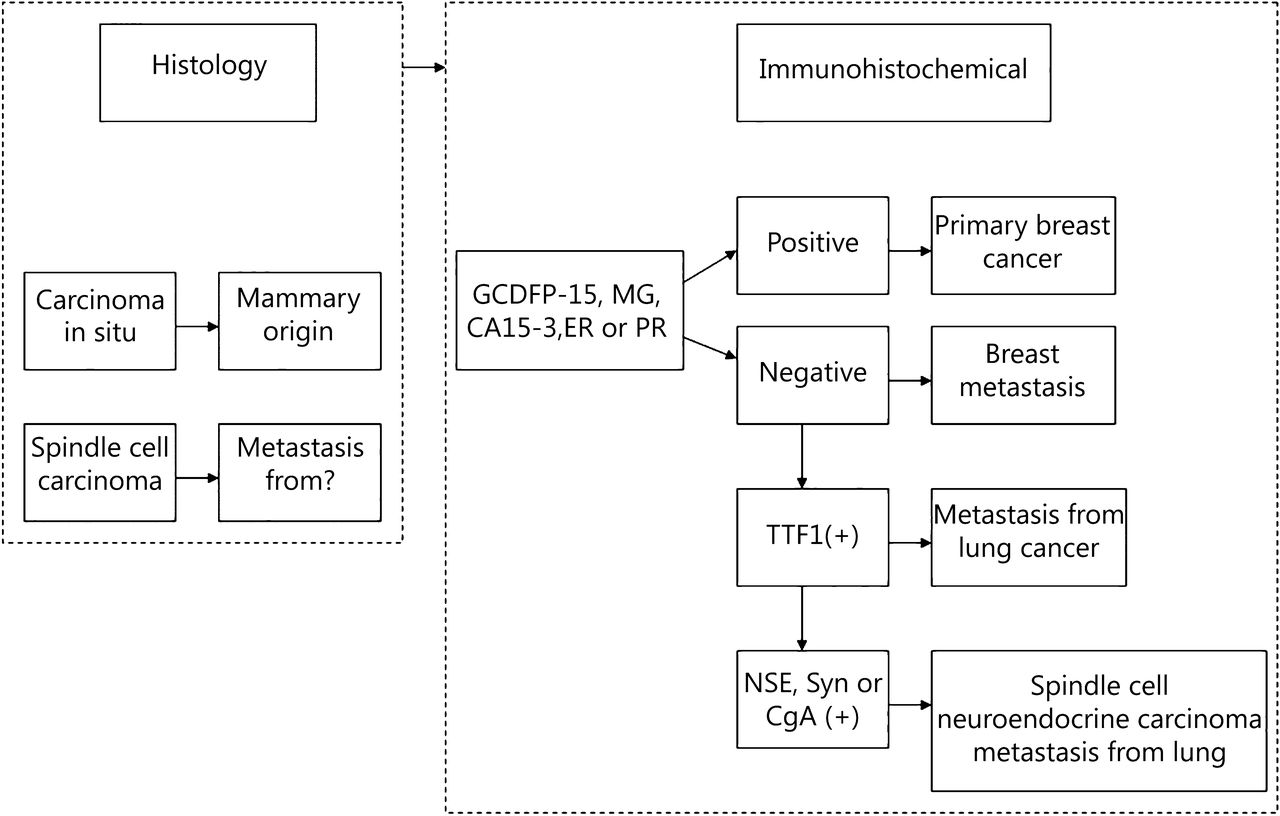
We report two patients with breast metastases from pulmonary adenocarcinoma: one patient was characterized by neuroendocrine cells and diagnosed consistently with primary tumor; another patient exhibited small cell lung carcinoma. Patients with breast metastases from pulmonary adenocarcinoma usually present multiple, superficial, and well-circumscribed lesions. Pathologists should consider this diagnosis if morphological characteristics are unusual for a primary mammary tumor. About two-thirds of the cases possibly show histological characteristics indicative of possible metastasis. In one-third of such cases, medical history is vital for differential diagnosis. Small cell carcinoma suggests a pulmonary origin. Carcinoma in situ suggests a mammary origin15. The distinction between metastases from lung adenocarcinoma and primary mammary adenocarcinoma may cause a significant diagnostic dilemma. As such, the contribution of immunohistochemistry to a correct diagnosis is crucial. For example, TTF1 is a useful marker of pulmonary adenocarcinoma with a reported frequency of 68% to 80%; however, no stains are positively detected in breast carcinoma25–27 except a single case published by Klingen et al.25. The mammary origin is supported by the expression of ER, GCDFP-15 and MG. ER and GCDFP-15 are expressed in 80% and 45% to 53% of breast carcinoma, respectively26,28. Studies have revealed that ER expression in lung adenocarcinoma is low (7.6% to 14.1%)26,29. Furthermore, GCDFP-15 is expressed in 5.2% to 15% of lung adenocarcinoma28,30. MG is expressed in 48% to 72.1% of mammary adenocarcinoma but stained negatively in pulmonary adenocarcinoma26,28,31. Many cases of primary and metastatic breast adenocarcinoma (including ductal and lobular) are K7+/K20−/K5/6−, which exhibits an important diagnostic value in combination with ER, PR and GCDFP-15 immunohistochemistry in differentiating a primary breast adenocarcinoma from an adenocarcinoma at another primary site32. Lung adenocarcinomas are K7+ whereas lung squamous cell carcinomas are usually K7−33. Lung neuroendocrine carcinomas (large cell neuroendocrine carcinoma and small cell carcinoma) are usually negative for K7 and K2034. The expression of NSE, Syn or CgA is indicative of carcinomas with neuroendocrine differentiation35. Hepatocellular carcinomas generally express K8 and K18 but are negative for K7, K19 and K2036. Consequently, it is important to use a panel of antibodies as no single marker is completely sensitive or specific.
Scholars do not prefer mastectomy, although local excision and systemic treatment are recommended for breast metastasis. In general, metastasis to the breast has been associated with poor prognosis in patients who die within a year of diagnosis6. Our these two patients remained alive for 7 and 8 months after they were diagnosed with primary lung tumor and breast metastasis, respectively. Hence, patients should be followed up continually.
We presented two patients who developed metastasis to the breast from lung cancer. This metastasis is a very rare occurrence, and the prognosis of these patients is poor. A combination of clinical history, image data and pathology may provide effective and robust measures for disease diagnosis than any single modality. A detailed examination of the breast mass and specific immunohistochemical analysis are necessary to distinguish a primary breast cancer from metastasis to the breast to avoid unessential mastectomy and provide appropriate systemic treatment because the recommended therapy is possibly different with considerably varying outcomes.
Acknowledgements
This work was supported by the National Natural Science Foundation of China (Grant No. 81172532) and the Program for Changjiang Scholars and Innovative Research Team in University (Grant No. TRT0743).
Footnotes
Conflict of interest statement No potential conflicts of interest are disclosed.
- Received April 15, 2014.
- Accepted July 13, 2014.
- Copyright: © 2014, Cancer Biology & Medicine
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC BY) 4.0, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.